Written by Steven Hansen
The U.S. new cases 7-day rolling average are 3.8 % LOWER than the 7-day rolling average one week ago. U.S. hospitalizations due to COVID-19 are now 13.2 % LOWER than the rolling average one week ago. U.S. deaths due to coronavirus are now 4.7 % HIGHER than the rolling average one week ago. Today’s posts include:
- U.S. Coronavirus New Cases are 51,204
- U.S. Coronavirus hospitalizations are at 47,352
- U.S. Coronavirus deaths are at 1,097
- U.S. Coronavirus immunizations have been administered to 21.7 % of the population
- The 7-day rolling average rate of growth of the pandemic shows new cases improved, hospitalizations unchanged, and deaths improved [note: this is a sign of trend reversal – could the new variants be impacting COVID case growth?>
- Pfizer-BioNtech Covid-19 vaccine less effective on obese people, finds study
- Older Heavier People May Be ‘Superspreaders’ of COVID-19
- Here is how Johnson & Johnson’s vaccine differs from Pfizer’s and Moderna’s
- Study backs link between Vitamin D and COVID-19 severity
- Why has coronavirus testing slumped in the U.S.? It’s complicated.
- US reports record number of variant coronavirus cases
- Is This Why “New COVID Cases” Are Crashing?
- The FDA authorizes another at-home Covid-19 antigen test
- The number of hospitals reporting full ICUs has fallen by nearly 50% since early January
- How to Use the Vaxxmax COVID Vaccine Website to Get Appointments Around the U.S.

The recent worsening of the trendlines for new cases is behind us which was attributed to going back to college/university, cooler weather causing more indoor activities, mutation of the virus, fatigue from wearing masks / social distancing, holiday activities, and some loosening of regulations designed to slow the coronavirus spread.
My continuing advice is to continue to wash your hands (especially after using the toilet as COVID first sheds in your stool), putting down the toilet seat (as flushing the toilet releases a plume), wear masks, avoid crowds, and maintain social distancing. No handwashing, mask, or social distancing will guarantee you do not get infected – but it sure as hell lowers the risk in all situations – and the evidence to-date shows a lower severity of COVID-19. In addition, certain activities are believed to carry higher risk – like being inside in air conditioning and removing your mask (such as restaurants, around your children/grandchildren, bars, and gyms). It is all about viral load – and outdoor activities are generally safe if you can maintain social distance. Finally, studies show eating right (making sure you are supporting your immune system) and adequate sleep increase your ability to fight off COVID.
include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus1.htm’); ?>
Hospitalizations Are The Only Accurate Gauge As Reporting Is Not Affected By Holidays
The 4 day Thanksgiving holiday period put the first wobble in the trends. Over weekends and holidays, the number of new cases and deaths decline. Over weekends, this is not a problem for week-over-week rolling averages as weekends are compared against the previous weekend. But when a holiday falls within a working week, a non-working day is compared to a working day which causes havok in the trends.
However, hospitalizations historically appear to be little affected by weekends or holidays – the daily counts do not vary significantly from day-to-day.
The hospitalization growth rate trend is improving.

For the Thanksgiving and the end of the year holiday period – roughly, it seems each appears to have added around 5 % to the rate of growth of new cases, hospitalizations, and deaths.
Historically, hospitalization growth follows new case growth by one to two weeks.
As an analyst, I use the rate of growth to determine the trend. But, the size of the pandemic is growing in terms of real numbers – and if the rate of growth does not become negative – the pandemic will overwhelm all resources.
The graph below shows the rate of growth relative to the growth a week earlier updated through today [note that negative numbers mean the rolling averages are LOWER than the rolling averages one week ago]. As one can see, the rate of growth for new cases peaked in early December 2020 for Thanksgiving, and early January 2021 for end of year holidays – and the rate of growth is now contracting.

In the scheme of things, new cases decline first, followed by hospitalizations, and then deaths.
It is up to each of our readers to protect themselves and others by washing hands, wearing a mask, avoiding crowds, and maintaining social distancing.
Will The New Variants Cause The Next Spike?
Maybe and maybe not. It all depends on vaccinations:
- the more people that are vaccinated reduces the pool of people that can be infected. Today we have removed over 22 % of the population from being infected which theoretically should reduce the infection rate by 22 % [it is unproven whether the vaccines prevent a vaccinated person from being a carrier of the virus even though showing no signs]. If the vaccines are shown to stop transmission, then in theory it would reduce the infection rate by double the percent vaccinated [in this case you prevent your own infection and do not pass it along to another].
- it is also unknown what the effective rate of the current vaccines is against mutations that seem to appear almost daily. As an example, if the effective rate drops to 60%, it means the 22 % reduction in the infection rate discussed above is almost cut in half. The South African and Brazilian variant is somewhat immune to the current vaccines.
- The pandemic should be over immediately if everyone could be vaccinated today. The problem is that every day brings a new mutation (which would not appear if the pandemic was stopped). The longer the immunization process takes – the more ineffective the vaccine will become.
- It is not clear whether the vaccine prevents those vaccinated from spreading the virus. It seems to be well documented that it normally stops the virus from taking hold and when it does not – the infection is mild.
Coronavirus News You May Have Missed
Here is how Johnson & Johnson’s vaccine differs from Pfizer’s and Moderna’s. – New York Times
Here is how they compare.
One shot instead of two
The Johnson & Johnson vaccine is administered in a single shot, while the Pfizer-BioNTech and Moderna vaccines are given in two shots several weeks apart.
The way it works
The Johnson & Johnson vaccine uses a different method to prime the body to fight off Covid-19: a viral vector called Ad26. Viral vectors are common viruses that have been genetically altered so that they do not cause illness but can still cause the immune system to build up its defenses. The Pfizer-BioNTech and Moderna vaccines use messenger RNA to do that.
How well it works
The Johnson & Johnson vaccine is rated as highly effective at preventing serious illness and death, as the Pfizer-BioNTech and Moderna vaccines are. It is also very effective at preventing milder illness, though a bit less so than those two. It appears to do well against the highly contagious B.1.351 variant, first identified in South Africa, that has given at least one other vaccine candidate trouble.
Storage and handling
The Johnson & Johnson vaccine does not have to be stored at extremely low temperatures like the Pfizer-BioNTech vaccine. It can safely be kept in an ordinary refrigerator for three months, much longer than the Moderna vaccine, which spoils after a month if not kept frozen.
Side effects
The Johnson & Johnson vaccine appears to be less prone than the Pfizer-BioNTech and Moderna vaccines to trigger the kinds of side effects that require monitoring after the injection, which may make it more suitable for use at drive-through vaccination sites. There have been reports that side effects tend to be felt more strongly after second doses, which the Johnson & Johnson vaccine does not require.
Is This Why “New COVID Cases” Are Crashing?
[editor’s note: this post is interesting but I do not buy that the fall is due to unreliable testing. The hospitalization graph we show in this post daily shows a dramatic fall in hospitalizations – and this has NOTHING to do with unreliable testing]
The scary red numbers are all going down. Check any newspaper or covid tracking website you want. Cases. Deaths. Hospitalisations. They’re all going down, sharply, and have been for weeks, especially in the US and UK.
So, why would that be?
Pundits across the media world have made suggestions – from vaccines to lockdowns – but there’s only one that makes any real sense.
IT’S NOT VACCINES
The assumption most people would make, and would be encouraged to make by the talking heads and media experts, is that the various “vaccines” have taken effect and stopped the spread of the “virus”.
Is this the case? No, no it’s not.
The decline started in mid-January, far too early for any vaccination program to have any effect. Many experts said as much:
Dr. Wafaa El-Sadr, professor of epidemiology and medicine at Columbia University’s Mailman School of Public Health, said the falling case numbers can’t be attributed to the COVID-19 vaccine, because not even a tenth of the population has been vaccinated, according to the CDC.
Further, the drop is happening simultaneously in different countries all around the world, and not every country is vaccinating at the same rate or even using the same vaccine. So no, the “vaccines” are not causing the drop.
IT’S NOT LOCKDOWN EITHER
Another suspect is the lockdown, with blaring propaganda stating that all the various government-imposed house arrests and “distancing” measures have finally had an impact.
That’s not it either.
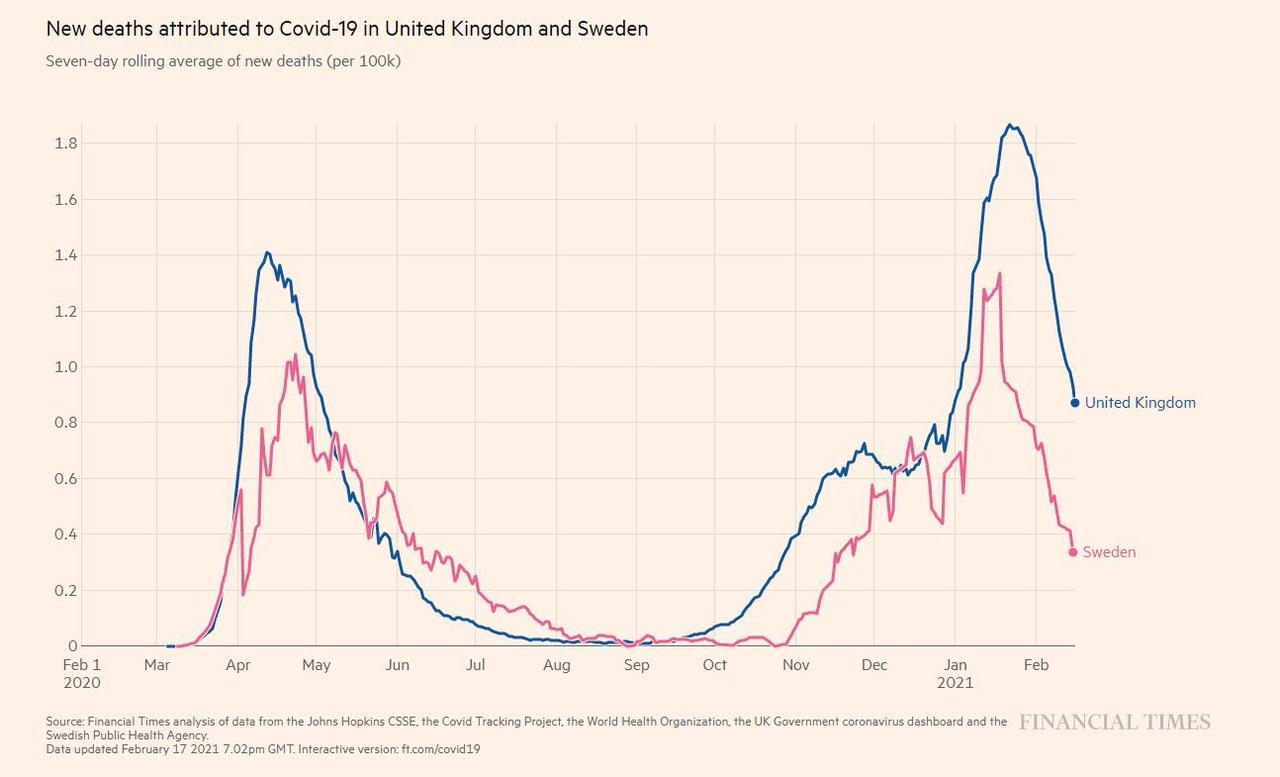
Sweden, famously, never locked down at all. Yet their “cases” and “Covid related deaths” have been dropping exactly in parallel with the UK:
Clearly, if countries that never locked down are also seeing declines in case numbers, the lockdown cannot be causing them.
So what is?
THE WHO PCR TEST GUIDELINES
Maybe for our answer, we should look at the date the decline started.
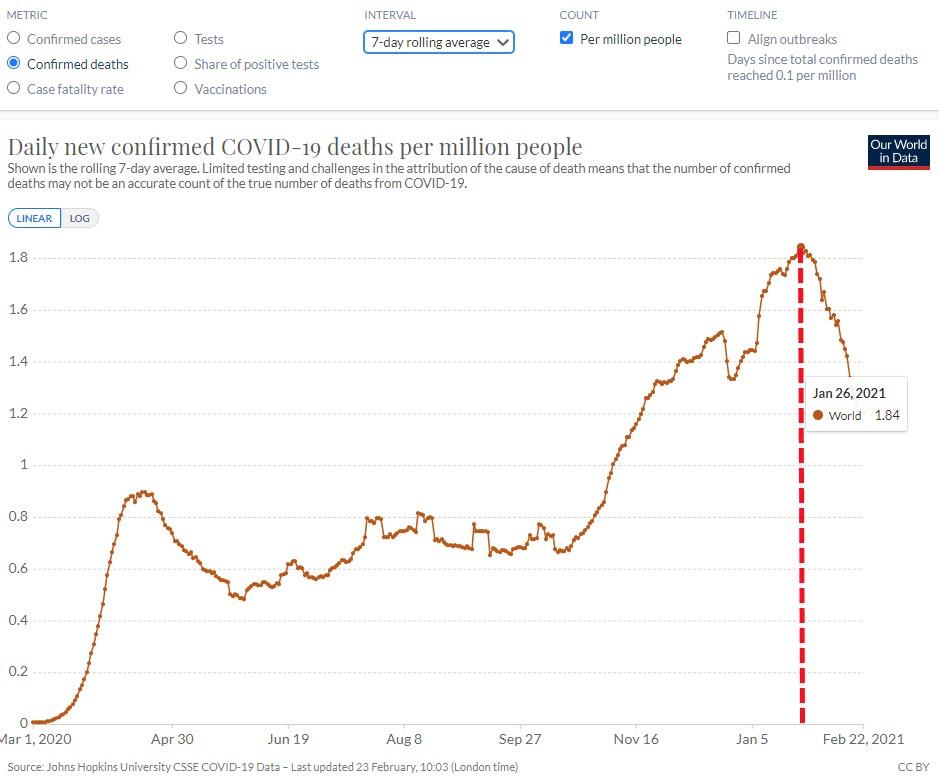
Observe this graph:
As you can see, the global decline in “Covid deaths” starts in mid-to-late January.
What else happened around that time?
Well, on January 13th the WHO published a memo regarding the problem of asymptomatic cases being discovered by PCR tests, and suggesting any asymptomatic positive tests be repeated.
This followed up their previous memo, instructing labs around the world to use lower cycle thresholds (CT values) for PCR tests, as values over 35 could produce false positives.
Essentially, in two memos the WHO ensured future testing would be less likely to produce false positives and made it much harder to be labelled an “asymptomatic case”.
In short, logic would suggest we’re not in fact seeing a “decline in Covid cases” or a “decrease in Covid deaths” at all.
What we’re seeing is a decline in perfectly healthy people being labelled “covid cases” based on a false positive from an unreliable testing process. And we’re seeing fewer people dying of pneumonia, cancer or other disease have “Covid19” added to their death certificate based on testing criteria designed to inflate the pandemic.

One year into pandemic, sky begins to clear over U.S. economy – Reuters
Despite the U.S. economy’s near miss with a depression last year and an ongoing coronavirus pandemic that has brought travel to a virtual halt, Jeff Hurst, the chief executive of vacation rental firm VRBO, sees a boom on the horizon.
“Every house is going to be taken this summer,” Hurst said, as the expected protection from vaccines arrives in step with warmer weather, unleashing a cooped-up population with record savings stashed away. “There’s so much built-up demand for it.”
That sort of bullish sentiment has increasingly taken root among executives, analysts and consumers who see the past year of comparative hibernation – from the government-ordered business closings last spring to continued risk avoidance by the public – giving way to a cautious re-emergence and green shoots in the economy.


Pfizer-BioNtech Covid-19 vaccine less effective on obese people, finds study – BusinessLine
A new study has revealed that the Pfizer-BioNtech COVID-19 vaccine might be less effective on obese people, media reports said.
The study carried out by a group of Italian researchers, suggested that obese healthcare workers who received the COVID-19 vaccine were not able to produce as many antibodies as their healthy peers.
The obese healthcare workers had only half the amount of antibodies produced by healthy workers after the administration of the second dose.
According to the study conducted by Aldo Venuti, from the Istituti Fisioterapici Ospitalieri in Rome, 99.5 per cent of these healthcare workers had developed an antibody response against the virus seven days after the second dose administration.
But this response was dissimilar to what obese people witnessed after the administration of both doses of the vaccine.
“Since obesity is a major risk factor for morbidity and mortality for patients with Covid-19, it is mandatory to plan an efficient vaccination programme in this subgroup,” Venuti said, as cited in the media reports.
He added: “Although further studies are needed, this data may have important implications to the development of vaccination strategies for Covid-19, particularly in obese people. If our data was to be confirmed by larger studies, giving obese people an extra dose of the vaccine or a higher dose could be options to be evaluated in this population.”
Study backs link between Vitamin D and COVID-19 severity
A retrospective study of elderly COVID-19 patients has concluded that vitamin D serum deficiency is associated with more severe lung symptoms, longer disease duration and higher risk of death.
The number of hospitals reporting full ICUs has fallen by nearly 50% since early January – USA Today
Detailed data released this week by the U.S. Department of Health and Human Services illustrates the impact of the COVID-19 pandemic on the nation’s hospitals.
From Olympic Medical Center in Port Angeles, Washington, to Sibley Memorial Center in Washington, D.C., USA TODAY found 175 hospitals reporting full intensive care units as of Feb. 25. A total of 302 hospitals reported more COVID-19 patients in the ICU compared with the previous week, and 493 had more COVID-19 patients overall.
Though still dire, these numbers have fallen drastically since the beginning of the year. The number of hospitals reporting full intensive care units has fallen by nearly 50% since early January, a USA TODAY analysis of HHS data shows. And the number of hospitals reporting intensive care units full of patients confirmed or suspected of having COVID-19 has fallen from 35 to four since the week of Jan. 8-14.
US reports record number of variant coronavirus cases – The Hill
The U.S. on Sunday reported an all-time high of 306 cases of coronavirus variants, with the majority concentrated in Florida, Michigan and Texas, USA Today reported.
The new cases included 104 new infections in Florida, for a total of 605 in that state; 85 in Michigan, for a total of 421; and 41 in Texas, for a total of 102. Although various new strains are known to be circulating in the U.S., the majority of the new and existing variant cases are the B.1.1.7. strain that originated in the United Kingdom. The Centers for Disease Control and Prevention (CDC) has said the British strain may become the most common in the country over the next month.
Overall coronavirus cases declined in February after reaching an all-time high in January, but there are signs the decline is slowing or reversing. The majority of states on Sunday reported rising case counts for the past week for the first time in more than a month.
Both the variants and the trends come as the U.S. continues administration of the coronavirus vaccine. Over the weekend, Johnson & Johnson began distribution of its shot after it received emergency-use authorization and became the third available vaccine.
Older Heavier People May Be ‘Superspreaders’ of COVID-19 – Medscape
People with higher body mass index (BMI) and older age are more likely to spread SARS-CoV-2 because they exhale more respiratory droplets, but a “nasal hygiene” product can reduce those, researchers say.
The study about age and BMI was published online February 9 in Proceedings of the National Academy of Sciences. It was conducted by David A. Edwards, Ph.D., founder and chief scientific officer of Sensory Cloud, Boston, Massachusetts, and formerly professor of bioengineering at Harvard University, Boston, and colleagues.
The results “raise the question, ‘What is causing some people to exhale many more respiratory droplets than other people?’ ” Edwards told Medscape Medical News. “This work shows that there are a few factors at least ― age, BMI, and particularly strong correlations with age times BMI and respiratory infection itself,” he noted.
Edwards’ company makes a product called FEND (“fast emergency nasal defence”) that is designed to suppress airway droplets in the nasal passages. It consists of a misting device and a calcium-enriched saline aerosol that is inhaled and lasts up to 6 hours.
He claims it may help to reduce the spread of COVID-19 and other respiratory infections, although other experts are not entirely convinced.
… In the new study, Edwards and colleagues measured exhaled respiratory particles in a total of 194 healthy persons at two different US sites and in eight nonhuman primates that had been experimentally infected with SARS-CoV-2.
Among the humans, those in the top 18% for the metric of BMI multiplied by age accounted for 80% of exhaled bioaerosols. In the animals, higher viral loads correlated with greater particle exhalation.
The study is the first to attribute COVID-19 “superspreader” capabilities to individual human characteristics, as opposed to events involving crowds or unmasked behaviors.
How to Use the Vaxxmax COVID Vaccine Website to Get Appointments Around the U.S. – Newsweek
With COVID-19 vaccines in high demand across the United States, finding a location to book a shot can be tricky.
In order to address this problem, software engineer and electronic musician Adam Freemer created a website tool to help people book vaccine appointments with select pharmacies.
“VaxxMax.com is a free, no sign-up national vaccine availability website tool built for one reason: to help get you vaccinated. It currently covers all Rite Aid and Walgreens locations nationwide (with more providers to come) and gives near real-time availability to help you find a location to schedule your vaccination,” Freemer wrote on the tool’s Facebook page.
“The tool is free but donations to cover hosting and development costs are welcome.”
In addition to Rite Aid and Walgreens, Freemer tweeted yesterday that he was adding “more providers currently as we speak.”
Why has coronavirus testing slumped in the U.S.? It’s complicated. – New York Times
Experts cited a number of factors that could be contributing to the slump:
Fewer exposures. Since daily tallies of new coronavirus infections have fallen sharply, fewer people may be having contacts that would prompt them to seek a test.
Less travel. The holiday rush is over, reducing the need for people to get tested before or after trips.
Bad weather. The severe storms and Arctic temperatures that battered much of the country, from Texas to the Northeast, caused many testing sites to close temporarily.
The vaccine rollout. Some states have shifted their limited public health resources, and their public messaging, toward vaccination efforts at the expense of testing.
Pandemic fatigue. Some experts worry the decline may be yet another symptom of public exhaustion and frustration with pandemic precautions and safety measures.
All those forces may be at play, said Dr. Jennifer Nuzzo of the Johns Hopkins Bloomberg School of Public Health: “My sense is that it’s probably that there are fewer options for testing, fewer communications about it, people may be perceiving that it’s less necessary — maybe they just don’t see the point any more.”
The FDA authorizes another at-home Covid-19 antigen test – CNN
The US Food and Drug Administration on Monday granted emergency use authorization to the Quidel QuickVue At-Home Covid-19 Test.
Dr. Jeff Shuren, director of the FDA’s Center for Devices and Radiological Health, said in a statement that “The FDA continues to prioritize the availability of more at-home testing options in response to the pandemic.”
Here are some key things to know about the at-home test:
- The test is authorized for at-home use once prescribed by a physician.
- The nasal swab test can be self-administered by people who are 14 years of age and older, or samples can be collected by an adult in children 8 years of age and older.
- The test is to be used within the first 6 days that someone is experiencing symptoms of Covid-19.
Rapid antigen tests have been shown to be less accurate than RT-PCR tests, which are considered the “gold-standard” of diagnostic testing.
In a press release, Quidel said the test can return results in as little as 10 minutes, and that positive test results match PCR tests 84.8% of the time; negative test results match PCR results 99.1% of the time.
The following are foreign headlines with hyperlinks to the posts
Modi is inoculated as the vaccination drive in India enters a new phase.
The Philippines begins its inoculation campaign, but public distrust runs deep.
Amid turmoil over elections, rising cases in Somalia fuel talk of a new lockdown.
The E.U. will propose a vaccine passport system for Europe.
Nordic nations tighten restrictions as cases surge
The following additional national and state headlines with hyperlinks to the posts
AstraZeneca has sold its stake in Moderna for more than $1 billion
Fauci warns about easing restrictions
Arab American COVID deaths counted as ‘white’
Asian Americans face hate crimes, attacks over COVID-19
Feeling unmotivated? You’re not alone. What to do.
Food Prices Are Soaring Faster Than Inflation and Incomes
$3 gasoline could be around the corner — unless OPEC and Russia start pumping more oil
The recent sharp decline in COVID-19 cases appears to have leveled off in the U.S., and more than half of states are showing increases in week-over-week case counts.
More than 2,400 reported cases of Covid variants in the US
Walmart drops $35 minimum on deliveries
White House: US will help Mexico after Americans vaccinated
Johnson & Johnson vaccine rollout begins with around 4 million doses
NBA calls off Raptors, Bulls game amid COVID-19 challenges
Plunging Demand for COVID-19 Tests May Leave US Exposed
House OKs $1.9 Trillion COVID Relief Package
RFK Jr. Would “Absolutely Not” Advise His Mom Ethel to Get COVID Vaccine
Fauci Urges Americans to Take 1st Available COVID Vaccine
California’s governor and legislature reach an agreement on a school-reopening plan.
Thousands of farmworkers are prioritized for vaccinations.
The British government was hunting on Monday for someone whose Covid-19 test sample came back positive for a concerning variant of the coronavirus first detected in Brazil, one of the first known instances of that variant in Britain.
Texas FEMA sites expected to receive 24,000 Johnson & Johnson vaccine doses today
US military has administered over 1 million Covid-19 vaccine doses
Johnson & Johnson working on booster for coronavirus variants
Johnson & Johnson will deliver 20 million vaccine doses in March and 100 million by June
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
February 2021 ISM and Markit Manufacturing Surveys Mixed
January 2021 Construction Spending Again Improves
Are COVID Vaccines Vegan? Should I Get One Anyway? An Ethicist Explains
Warning to Readers
The amount of politically biased articles on the internet continues to increase. And studies and opinions of the experts continue to contradict other studies and expert opinions. Honestly, it is difficult to believe anything anymore.

I assemble this coronavirus update daily – sifting through the posts on the internet. I try to avoid politically slanted posts (mostly from CNN, New York Times, and the Washington Post) and can usually find unslanted posts on that subject from other sources on the internet. I wait to publish posts on subjects that I cannot validate across several sources. But after all this extra work, I do not know if I have conveyed the REAL facts. It is my job to provide information so that you have the facts necessary – and then it is up to readers to draw conclusions.
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19 when recovering from COVID-19. Herd immunity does not look like an option without immunization although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a significantly higher death rate as there is relatively few hospitalizations and deaths in younger age groups..
- There are at least 8 strains of the coronavirus. New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
What we do or do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work. Unfortunately, early in the pandemic, many health experts — in the U.S. and around the world — decided that the public could not be trusted to hear the truth about masks. Instead, the experts spread a misleading message, discouraging the use of masks.
- Current thinking is that we develop 5 months of immunity from further COVID infection.
- The Moderna and Pfizer vaccines have an effectiveness rate of about 95 percent after two doses. That is on par with the vaccines for chickenpox and measles. The 95 percent number understates the effectivenessas it counts anyone who came down with a mild case of Covid-19 as a failure. But turning Covid into a typical flu — as the vaccines evidently did for most of the remaining 5 percent — is actually a success. Of the 32,000 people who received the Moderna or Pfizer vaccine in a research trial, only one contracted a severe Covid case.
- To what degree do people who never develop symptoms contribute to transmission? Research early in the pandemic suggested that the rate of asymptomatic infections could be as high as 81%. But a meta-analysis, which included 13 studies involving 21,708 people, calculated the rate of asymptomatic presentation to be 17%.
- The accuracy of rapid testing is questioned – and the more accurate test results are not being given in a timely manner.
- Can children widely spread coronavirus? [current thinking is that they are a minor source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- Air conditioning contributes to the pandemic spread.
- It appears that there is increased risk of infection and mortality for those living in larger occupancy households.
- Male patients have almost three times the odds of requiring intensive treatment unit (ITU) admission compared to females.
- Outdoor activities seem to be a lower risk than indoor activities.
- Will other medical treatments for Covid-19 ease symptoms and reduce deaths? So far only remdesivir, Bamlanivimab,
and Regeneron) are approved for treatment. What drugs work?
Arthritis drugs tocilizumab and sarilumab could cut relative risk of death of those in intensive care by 24%
- A current scientific understanding of the way the coronavirus works can be found [here].
There is now a vaccine available – the questions remain:
- how effective it will be in the general population,
- will there be any permanent side effects that will appear months from now,
- how long immunity will last [we can currently say we do not know if it will last more than 4 months],
- there is no evidence the vaccine will block transmission
Heavy breakouts of coronavirus have hit farmworkers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>





