Written by Steven Hansen
The U.S. new cases 7-day rolling average is 5.1 % HIGHER than the 7-day rolling average one week ago. U.S. hospitalizations due to COVID-19 are now 4.3 % HIGHER than the rolling average one week ago. U.S. deaths due to coronavirus are now 5.2 % HIGHER than the rolling average one week ago. Today’s posts include:
- U.S. Coronavirus New Cases are 160,606
- U.S. Coronavirus hospitalizations are at an elevated 125,057 (for the next 9 days this is the number to watch as new cases and deaths will not be accurately reported)
- U.S. Coronavirus deaths are at an elevated 2,051
- U.S. Coronavirus immunizations have been administered to 0.8% of the population
- The 7-day rolling average rate of growth of the pandemic shows new cases worsened, hospitalizations worsened, and deaths worsened
- US to test whether Covid-19 vaccines are effective against South African coronavirus variant
- Turkey becomes the 33rd country to find the virus variant first identified in Britain
- Here’s what scientists know about how the coronavirus variant spreads
- What we’ve learned about how our immune system fights COVID-19
- COVID Clot Prevention Evidence Beginning to Bud
- Can New York force you to get a coronavirus vaccine?
- They spent 12 years solving a puzzle. It yielded the first COVID-19 vaccines
- The legacy of 2020: Riches for the wealthy and White, financial pain for others
​
The recent worsening of the trendlines for new cases should be attributed to going back to college/university, cooler weather causing more indoor activities, possible mutation of the virus, fatigue from wearing masks / social distancing, holiday activities, political rallies / voting, and continued loosening of regulations designed to slow the coronavirus spread.
My continuing advice is to continue to wash your hands (especially after using the toilet as COVID first sheds in your stool), putting down the toilet seat (as flushing the toilet releases a plume), wear masks, avoid crowds, and maintain social distancing. No handwashing, mask, or social distancing will guarantee you do not get infected – but it sure as hell lowers the risk in all situations – and the evidence to-date shows a lower severity of COVID-19. In addition, certain activities are believed to carry higher risk – like being inside in air conditioning and removing your mask (such as restaurants, around your children/grandchildren, bars, and gyms). It is all about viral load – and outdoor activities are generally safe if you can maintain social distance. Finally, studies show eating right (making sure you are supporting your immune system) and adequate sleep increase your ability to fight off COVID.
include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus1.htm’); ?>
Hospitalizations (grey line) and Mortality (green line)
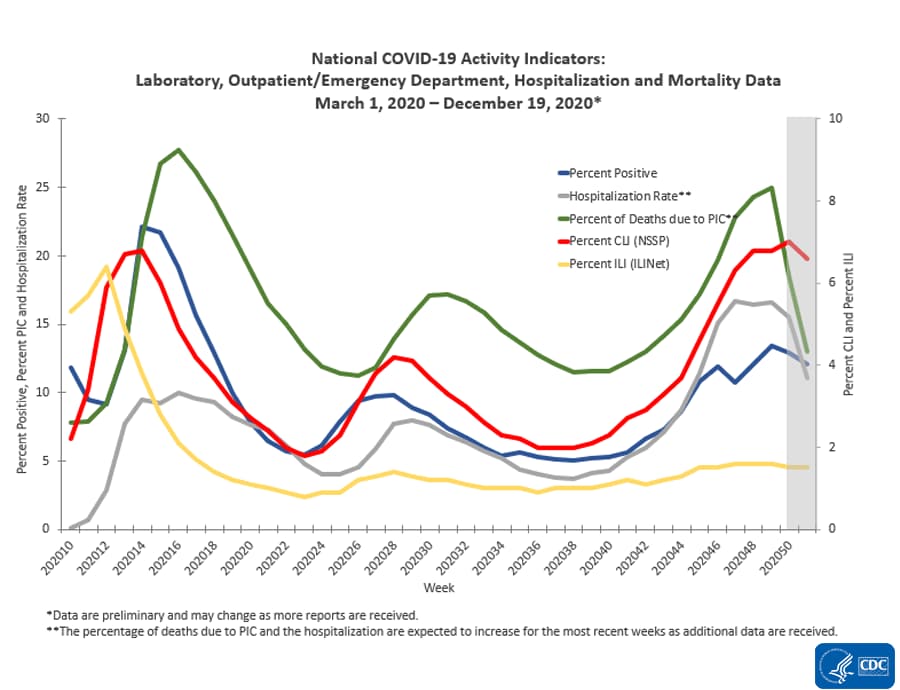
source: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html
The Impact of Holidays – Hospitalizations Are The Only Accurate Gauge As Most Reporting Is Not Timely
The 4 day Thanksgiving holiday period put a wobble in the trends. Over weekends and holidays, the number of new cases and deaths decline. Over weekends, this is not a problem for week-over-week rolling averages as weekends are compared against the previous weekend. But when a holiday falls within a working week, a non-working day is compared to a working day which causes havok in the trends. Now we are faced with the end of the year holiday season which means reporting is sporadic and numbers will initially look good – and then as the holidays end and the reporting catches up, the numbers will look terrible. In addition, family gatherings and travel will cause more virus transmission.
However, hospitalizations historically appear to be little affected by weekends or holidays – the daily counts do not vary significantly from day-to-day.
The hospitalization growth rate trend is growing at an ever slowing growth rate which is all good news as it means the number of beds needed is currently growing around 4 % every week.

The above graph demonstrates in the last week hospitalization rate of growth has been relatively steady. We have seen that the size of the impact of commingling and travel over the Thanksgiving holiday period – roughly, it seems to have added around 5 % to the rate of growth of new cases, hospitalizations, and deaths.
Historically, hospitalization growth follows new case growth by one to two weeks.
As an analyst, I use the rate of growth to determine the trend. But, the size of the pandemic is growing in terms of real numbers – and if the rate of growth does not become negative – the pandemic will overwhelm all resources.
The graph below shows the rate of growth relative to the growth a week earlier updated through today [note that negative numbers mean the rolling averages are LOWER than the rolling averages one week ago]. As one can see, the rate of growth for new cases peaked in early December 2020 ago and the rate of growth has been decelerating since.

This graph is currently demonstrating that the actions to contain the pandemic are slightly working – but the rate of growth improvement is too slow as we are still seeing some record numbers. In the scheme of things, new cases decline first, followed by hospitalizations, and then deaths.
It is up to each of our readers to protect themselves and others by washing your hands, wearing a mask, avoiding crowds, and maintaining social distancing.
Likely There Will Be A Pandemic Surge After New Years
The “experts” will tell you they told you so – and you should have stayed at home instead of traveling to be with the people you care about. And there is some truth in this opinion.
But there will be no way to accurately understand the impact of the holidays because there are new mutant strains of the coronavirus that are more transmissible.
To gauge the impact of anything, you change ONLY ONE variable at a time (and hopefully in a controlled environment). There are now two variables in play – and it is nearly impossible to separate the impact of each.
Coronavirus News You May Have Missed
What we’ve learned about how our immune system fights COVID-19 – National Geographic
Twelve months of study have shown that our bodies, in many cases, develop a robust and persistent immune response to SARS-CoV-2, but for some people with severe cases, it can go haywire and hurts more than helps.
Our fundamental comprehension of immune responses to the coronavirus has grown significantly, but more questions-like the longevity of immunity-are still to be answered, especially amid concerns that mutations may help SARS-CoV-2 evade our immunological defenses. With vaccination on the horizon for many at-risk individuals, the immune response’s intricacies are even more critical to understand
… In a pivotal paper in June, researchers showed for the first time that recovered patients made not only coronavirus-specific antibodies-proteins designed to glom on and often neutralize an invader-but also elicited strong levels of killer T cells and helper T cells. Killer T cells recognize and destroy your own infected cells, an intentional bout of collateral damage intended to prevent a virus’s spread. Meanwhile, helper T cells aid that process and coordinate the maturation of antibodies.
These were encouraging results, and more were on the way. Though there was much talk of how recovered patients developed antibodies, nobody had actually shown that the presence of these proteins protected against infection until University of Washington virologist Alex Greninger and colleagues devised a natural experiment.
As part of their ongoing COVID-19 testing program, they performed screening for a commercial fishing boat, collecting blood samples before and after the voyage to track antibodies. Most of the 122 people on the fishing boat tested positive for the coronavirus on the return to shore-but none of the three crew members whose blood had antibodies against SARS-CoV-2 before departure were infected on the trip. Thanks to a bit of luck and clever design, the published study was the first to show that having antibodies likely protects from infection.
The Bad
Not everyone has a light case of COVID-19 with a lasting immune response-as evidenced by the grim figures of hospitalizations and deaths worldwide. The United States is experiencing twice as many hospitalizations now than at any other time in the pandemic. In severe cases, the immune system often goes haywire and causes more problems than it solves.
“It’s happening because the virus screwed up the type I interferon system,” Pillai says. “So, now you don’t get proper germinal centers, and those who do, it’s kind of wimpy germinal centers. So then at the end of the day, you don’t get the best, longest-lived antibody response.”
[editor’s note: This post is worth a full read]
Coronavirus closure is ‘nuclear bomb’ – German researcher – The Jerusalem Post
“The higher the number of people surrounding the infected person, the more the virus will spread,” explained Prof. Andrei Sommer.
Partial lockdowns could lead to an explosion in coronavirus cases, according to a top German researcher.
That is because the more people are in fewer places in less time, the more likely they are to pass on the virus, said Prof. Andrei Sommer, a visiting professor at Isra University in Jordan and formerly of the University of Ulm, in an interview with The Jerusalem Post.
He compared the results of partial lockdowns to a nuclear explosion.
The immense destructive power of atomic weapons is the result of a sudden release of energy produced by splitting the nuclei of the fissile elements making up the bombs’ core, according to the Atomic Heritage Foundation in an article about the science behind the atomic bomb. In order to detonate an atomic weapon, you need a critical mass of fissionable material. The more you have, the greater the odds that an explosion will occur.
“The critical mass is the number of people in a store at a certain time, which in a particle lockdown is compressed,” Sommer explained. “The neutrons are the people among them who are infected.
“The higher the number of people surrounding the infected person, the more the virus will spread,” he continued, “and each who is newly infected, infects other people – and this is the chain reaction in the nuclear bomb.”
… According to Sommer, the root cause of the dramatic increase in coronavirus infections in Germany and Israel in recent weeks is a result of the partial lockdown.
“By closing all shops except for three – supermarkets, gas stations and pharmacies – you are putting more people into smaller spaces per day,” Sommer said of the situation in his hometown.
US to test whether Covid-19 vaccines are effective against South African coronavirus variant – CNN
Scientists are studying whether a new variant of the novel coronavirus found in South Africa will pose a threat to existing vaccines, Dr. Anthony Fauci told CNN Friday.
“The proof of the pudding is we have to test it, and that is what is happening now, testing the strain found in South Africa against the antibodies produced by the vaccines. We don’t have that answer, but I am sure that answer is forthcoming soon,” Fauci said.
Fauci, director of the National Institute of Allergy and Infectious Diseases, said scientists in South Africa are testing to see if the vaccines are effective against the variant, and that testing is also happening – or will happen soon – in the US.
“I don’t know whether it’s going to be Monday or Tuesday, and there are a lot of groups that are doing it,” he said.
Fauci said Wednesday that Covid-19 vaccines should be effective against a new strain of the virus found in the UK.
The South African variant has been traced back to about Nov. 20, according to Tulio de Oliveira, the virologist who first identified it. It has 22 significant changes from previous strains of the coronavirus, and the UK strain has 17 mutations. Both are an unusually high number of mutations, and some of them are related to the spike proteins found on top of the virus, which is the target for antibodies generated by the vaccines.
Citing incoming travelers, Turkey becomes the 33rd country to find the virus variant first identified in Britain. – New York Times
Turkey slammed its doors to travelers from Britain on Friday, saying that it had found 15 infections with the new, more transmissible variant of the virus that first emerged in England. All were among recent arrivals from the United Kingdom.
Turkey’s health minister, Fahrettin Koca, issued a statement saying that the 15 people infected with the variant were in isolation and that their contacts were being traced and placed under quarantine. In countrywide checks, the statement said, the virus had not been detected in anyone other than travelers who arrived from Britain.
The finding brings the number of countries that have detected the variant to at least 33 since Britain announced finding it on Dec. 8, and the number of countries barring travelers arriving from Britain to more than 40. Some countries are also imposing restrictions on travelers, including U.S. citizens, who in recent weeks visited the countries where the variant has been detected.
The Philippines expanded restrictions on travelers from Britain and 18 other countries, adding the United States after a third state, Florida, reported an infection involving the variant. Many countries have already restricted travel from the United States because of its staggering number of infections – the most in the world.
The legacy of 2020: Riches for the wealthy and White, financial pain for others – CNBC
- The Covid recession, and the extreme inequality it wrought, will be among 2020s legacies.
- Rich, White and college-educated Americans saw jobs recover quickly, and their wealth balloon as the stock market and housing prices reached new highs.
- Racial minorities, low earners, women and those without a college degree were more likely to be unemployed and fall into poverty.
COVID Clot Prevention Evidence Beginning to Bud – MedPage
Clotting problems with severe COVID-19 became clear in the early days of the pandemic; now at around the 1-year mark of the first cases, research is just beginning to reveal what prophylactic strategies are best.
… clinical trials aimed at preventing these clots struggled. “I would have wished we had the results by now; part of the challenge is the disease came in waves,” Behnood Bikdeli, MD, of Brigham and Women’s Hospital and Harvard Medical School in Bosto noted.
The small phase II HESA COVID trial made it through, finding that therapeutic-level dosing of enoxaparin (Lovenox) improved respiratory outcomes in severe COVID-19. Some other trials with even modestly larger samples weren’t so lucky against rapidly shifting surges.
Interim analysis of only the largest randomized trial platforms have started to yield results on antithrombotic use for COVID-19 now in December.
Three adaptive platform partner trials — ACTIV-4, REMAP-CAP, and ATTACC — just halted therapeutic anticoagulation for prophylactic use in ICU patients after interim data showed futility in seeking a reduction in need for organ support and possible safety concern.
“It is terrific gain of knowledge to have results from randomized trials, even if they have to be stopped early,” said Stephan Moll, MD, a hematologist-oncologist involved in setting the prophylaxis protocols for the University of North Carolina at Chapel Hill. “This is refreshing news after all the retrospective, limited data of the first 9 months of the COVID-19 pandemic.”
ACTIV-4, REMAP-CAP, and ATTACC data are “urgently” undergoing additional analyses to be made available as soon as possible, according to trial leadership. Non-ICU subgroups, and a range of other treatment arms in those trials, are also ongoing.
They spent 12 years solving a puzzle. It yielded the first COVID-19 vaccines. – National Geographic
Long before anyone knew of SARS-CoV-2, a small band of government and university scientists uncovered a prototypical key that unlocked life-saving immunizations.
JASON MCLELLAN WAS wandering around a ski shop of Utah’s Park City Mountain Resort, waiting for his new snowboarding boots to be heat-molded to his size-nine feet, when his smartphone rang. It was Barney Graham, deputy director of the National Institute of Allergy and Infectious Diseases Vaccine Research Center.
Two days earlier, the World Health Organization had announced that several unidentified pneumonia-like cases had been reported in Wuhan, China. People were fatigued and feverish, with dry coughs and headaches. These symptoms weren’t unusual for early January, but some people were short of breath, and a few felt like they’d been hit by a train.
Graham told McLellan, a structural virologist at the University of Texas at Austin, that the ailment appeared to be a beta-coronavirus, meaning it fell into the genus of viruses that causes severe acute respiratory syndrome (SARS). He asked McLellan: “Are you ready to get back in the saddle?”
This duo was part of a small band of government and university scientists who had spent more than a decade cracking a complex viral puzzle-and their skills were needed once more. Their years of sleuthing and innovating ultimately contributed a microscopic but critical piece to the most promising candidates for COVID-19 vaccines. Two already authorized in the U.S. use their discovery, as do at least two other top contenders.
Their solution? Tweaking a shape-shifting protein to make it sit still.
[editor’s note: this is only the beginning of this comprehensive post which deserves a full read]
Here’s what scientists know about how the coronavirus variant spreads. – New York Times
The new variant, known as B.1.1.7, seems to infect more people than earlier versions of the coronavirus, even when the environments are the same.
Scientists initially estimated that the new variant was 70 percent more transmissible, but a recent modeling study pegged that number at 56 percent. Once researchers sift through all the data, it’s possible that the variant will turn out to be just 10 to 20 percent more transmissible, said Trevor Bedford, an evolutionary biologist at the Fred Hutchinson Cancer Research Center in Seattle.
Even so, Dr. Bedford said, it is likely to catch on rapidly and become the predominant form in the United States by March.
So far, at least, the variant does not seem to make people any sicker or lead to more deaths. Still, there is cause for concern: A variant that is more transmissible will increase the death toll simply because it will spread faster and infect more people.
Some preliminary evidence from Britain suggests that people infected with the new variant tend to carry greater amounts of the virus in their noses and throats than those infected with previous versions.
That finding offers one possible explanation for why the new variant spreads more easily: The more virus that infected people harbor in their noses and throats, the more they expel into the air and onto surfaces when they breathe, talk, sing, cough or sneeze.
With previous versions of the virus, contact tracing suggested that about 10 percent of people who have close contact with an infected person – within six feet for at least 15 minutes – inhaled enough virus to become infected.
… The vast majority of mutations provide no advantage to the virus and die out. But mutations that improve the virus’s fitness or transmissibility have a greater chance to catch on.
At least one of the 17 new mutations in the variant contributes to its greater contagiousness. The mechanism is not yet known. Some data suggest that the new variant may bind more tightly to a protein on the surface of human cells, allowing it to more readily infect them.
[editor’s note: also read UK variant coronavirus strain is significantly more transmissible – study and New Covid-19 Strains: What Scientists Know About Coronavirus Variants]
Can New York force you to get a coronavirus vaccine? – Syracuse
The question on government mandates during the pandemic always comes down to a balance between personal liberty and public health, said Stewart Schwab, law professor at Cornell University.
While coronavirus is deadlier than the common flu, it’s not a near-death sentence, like Ebola, for example.
A virus that killed 25% of those infected might warrant a stay-at-home order for anyone without a vaccination, Schwab said. But the coronavirus likely doesn’t meet that bar.
On the other hand, mandates regarding masks, testing and crowd sizes have been deemed reasonable: They’re somewhat intrusive, but not overboard considering the scientific evidence of the virus’s mortality rate.
“State governments have wide powers – general police powers – in times of crisis,” Schwab said. “Public health is classic example of use of police powers.”
So could the government make it so difficult to live daily life that vaccination seemed necessary? Perhaps.
Government action is typically presumed to be reasonable; a challenge to a government mandate requires proof that the action isn’t reasonable, Schwab said.
The following are foreign headlines with hyperlinks to the posts
More than 2,500 attend illegal New Year’s rave in France
More than 1,000 fines issued as illegal rave party ends in French countryside
Bangkok closes schools for two weeks to stem COVID-19 spread
Bangkok closes bars and entertainment venues
US travelers banned from Philippines starting Sunday
Britain authorizes mix-and-match vaccinations, but experts warn vaccines may not be interchangeable.
U.K. is in the ‘eye of the storm’ as coronavirus cases surge
South Korea extends gatherings limit nationwide as Covid-19 cases continue to spike
Japan has a record number of Covid-19 patients in serious condition
Israel vaccinates a million against COVID in less than two weeks
A nursing home in Belgium had a holiday party. It led to 27 coronavirus deaths.
India approves AstraZeneca’s COVID-19 vaccine
The following additional national and state headlines with hyperlinks to the posts
COVID-19 is taking a heavy toll in America’s mental health-care deserts
U.S. Surpasses 20 Million Confirmed Coronavirus Cases
Hundreds attend evangelist singer’s NYE concert in LA despite skyrocketing COVID-19 cases
Frustrations flare as $2,000 checks blocked for fourth straight day
Delta CEO predicts positive cash flow by spring
Nancy Pelosi’s Home Graffitied Over ‘$2K’ Stimulus Checks, Pig’s Head Left
Yoga Studio Allegedly Using Religious Exemption to Avoid COVID-19 Closures
Video Shows Gay Puerto Vallarta Boat Cruise Sinking Amid Worsening Pandemic
U.S. Ushers in New Year With 20M COVID Cases, 25 % of World’s Total
FL Gov Says He’s Not Taking COVID Vaccine Ahead of Seniors
Virginia State Senator Ben Chafin has died from Covid-19-related causes.
U.S. airlines’ 2020 losses expected to top $35 billion in dismal pandemic year
Tourists still flocking to South Florida despite record coronavirus numbers
Cleveland Browns reopen facility after no new positive coronavirus tests
Hundreds of thousands more US Covid deaths possible amid vaccine chaos
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
Fewer Job Seekers Relocating In Q3
The Impact Of The Pandemic And The Feds Muni Program On Illinois Muni Yields
Reclaiming Our World Post-2020
Medical Spending, Bequests, And Asset Dynamics Around The Time Of Death
Infographic Of The Day: The Economic Impact Of COVID-19
The Fractal Biology Of Plague And The Future Of Civilization
A Year Of Blursdays: How Coronavirus Distorted Our Sense Of Time In 2020
Warning to Readers
The amount of politically biased articles on the internet continues to increase. And studies and opinions of the experts continue to contradict other studies and expert opinions. Honestly, it is difficult to believe anything anymore. A study usually cannot establish cause and effect – but only correlation. Be very careful what you believe about this pandemic.

I assemble this coronavirus update daily – sifting through the posts on the internet. I try to avoid politically slanted posts (mostly from CNN, New York Times, and the Washington Post) and can usually find unslanted posts on that subject from other sources on the internet. I wait to publish posts on subjects that I cannot validate across several sources. But after all this extra work, I do not know if I have conveyed the REAL facts. It is my job to provide information so that you have the facts necessary – and then it is up to readers to draw conclusions.
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19 when recovering from COVID-19. Herd immunity does not look like an option without immunization although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a significantly higher death rate as there is relatively few hospitalizations and deaths in younger age groups..
- There are at least 8 strains of the coronavirus. New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
What we do or do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work.
- Do we develop lasting immunity to the coronavirus? Another coronavirus – the simple cold – does not develop long term immunity. However, How Many Americans Are Immune From COVID? Research into the coronavirus is running way behind the need for answers. Whilst we strive for herd immunity through vaccination – we lack an understanding of the general immunity people might have to the pandemic. This will affect the point herd immunity can be reached. The following articles discuss immunity: Can the Common Cold Help Protect You from COVID-19?, Does the Common Cold Protect You from COVID-19?, Immune cells for the common cold may recognize SARS-CoV-2
- To what degree do people who never develop symptoms contribute to transmission? Research early in the pandemic suggested that the rate of asymptomatic infections could be as high as 81%. But a meta-analysis, which included 13 studies involving 21,708 people, calculated the rate of asymptomatic presentation to be 17%.
- The accuracy of rapid testing is questioned – and the more accurate test results are not being given in a timely manner.
- Can children widely spread coronavirus? [current thinking is that they are a minor source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- Air conditioning contributes to the pandemic spread.
- It appears that there is increased risk of infection and mortality for those living in larger occupancy households.
- Male patients have almost three times the odds of requiring intensive treatment unit (ITU) admission compared to females.
- Outdoor activities seem to be a lower risk than indoor activities.
- Will other medical treatments for Covid-19 ease symptoms and reduce deaths? So far only remdesivir, Bamlanivimab,
and Regeneron) are approved for treatment. What drugs work?
- A current scientific understanding of the way the coronavirus works can be found [here].
There is now a vaccine available – the questions remain:
- how effective it will be in the general population,
- will there be any permanent side effects that will appear months from now,
- how long immunity will last [we can currently say we do not know if it will last more than 4 months],
- there is no evidence the vaccine will block transmission
Heavy breakouts of coronavirus have hit farmworkers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>





