Written by Steven Hansen
The U.S. new cases 7-day rolling average is 16.5 % HIGHER than the 7-day rolling average one week ago. U.S. deaths due to coronavirus are now 14.2 % HIGHER than the rolling average one week ago. At the end of this post is a set of interactive graphs and tables for the world and individual States – as well as today’s headlines which include;
- Global daily new coronavirus cases continue at record levels
- The U.S. again reported one of its highest daily case totals since the start of the pandemic.
- Weekly COVID-19 metrics worsened
- Slow Motion Sneeze in 4K
- Universal Mask Wearing Could Save Some 130,000 Lives In The U.S., Study Suggests
- Wanted: Online gamers to help build a more stable Covid-19 vaccine
- Home tests could help in the fight against the coronavirus. So where are they?
- Fast, cheap, accurate: Researchers pin hopes on Nobel Prize-winning CRISPR-technology tests to detect coronavirus
- In coronavirus testing, false positives are more hazardous than they might seem
- Musicians Improvise Masks for Wind Instruments to Keep the Band Together

The recent worsening of the trendlines for new cases should be attributed to going back to college/university, cooler weather causing more indoor activities, fatigue from wearing masks / social distancing, holiday activities, and continued loosening of regulations designed to slow the coronavirus spread.
My continuing advice is to continue to wash your hands, wear masks, avoid crowds, and maintain social distancing. No handwashing, mask, or social distancing will guarantee you do not get infected – but it sure as hell lowers the risk in all situations – as the evidence to-date shows a lower severity of COVID-19. In addition, certain activities are believed to carry higher risk – like being inside in air conditioning and removing your mask (such as restaurants, around your children/grandchildren, bars, and gyms). It is all about viral load – and outdoor activities are generally safe.
The daily number of new cases in the U.S. is remaining stubbornly and embarrassedly high – and is currently increasing.
The following graphs show the 7-day rolling average for new coronavirus cases and deaths have been updated through 25 October 2020:


z coronavirus.png
Hospitalizations (grey line) and Mortality (green line) For Week ending 17OCT2020
source: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html
Coronavirus Statistics For 25 October 2020 |
| U.S. Only | Global | U.S Percentage of Total | ||||
| Today*** | Cumulative | Today*** | Cumulative | Today | Cumulative | |
| New Confirmed Cases | 67,139 | 8,580,000 | 421,422 | 42,760,000 | 15.9% | 20.1% |
| Deaths** | 904 | 224,899 | 5,938 | 1,150,000 | 15.2% | 19.6% |
| Mortality Rate | 1.3% | 2.6% | 1.4% | 2.7% | ||
total COVID-19 Tests per 1,000 people | 2.23* | 415.63* | ||||
Source: EU CDC – The data insignificantly varies from the data produced by Johns Hopkins
* as of 20 Oct 2020
** evidently several States included “probable” deaths today in the number
*** red color indicates record number
Slow Motion Sneeze in 4K – The Slow Mo Guys with Dr Anthony Fauci
Somethings were never meant to be seen at 1000fps in 4K. I’d include this subject as one of them. Gav coughs, sneezes and talks in ultra backlit slow motion to illustrate the importance of wearing masks to prevent aerosolized particles from blasting out of your face holes. Who better to ask about the subject than Dr Anthony Fauci of the National Institute of Allergy and Infectious
A Review Of This Past Week
New coronavirus cases in the U.S. have now surged to levels not seen since the beginning of August whilst global new cases are historically high.

Deaths due to coronavirus grew this past week in the U.S. and globally.

The coronavirus infection fatality rate worsened in the U.S. and globally.

Econintersect published two summary posts for coronavirus news this past week:
Is The Light At The End Of The Tunnel A COVID-19 Vaccine?
I want my life to return to pre-pandemic normality. Months ago, I believed a vaccine would put an end to the pandemic – much like earlier vaccines used to combat measles, mumps, polio, and chickenpox which pretty much did their jobs to knock out these pandemics.
| Polio Virus | Measles | Mumps | chickpox |
 |  |  |  |
It is possible for a pandemic to vanish – but COVID-19 now has been with us a little short of one year – and it seems to be gaining strength. My money is on COVID-19 being endemic like the flu and the common cold. We have learned much about the illness, but nowhere near enough to effectively treat the illness once one is infected – and a potential vaccine is months away. We are hanging our hopes on a vaccine to end this pandemic.
A vaccine’s purpose is to create herd immunity. There are just two ways to achieve herd immunity: the vast majority of the population either gets infected or gets vaccinated. Herd immunity is what ends pandemics.
But COVID-19 is different from other viruses we have conquered. Per Wikipedia:
Coronaviruses are a group of RNA viruses that cause diseases in mammals and birds. In humans and birds, they cause respiratory tract infections that can range from mild to lethal. Mild illnesses in humans include some cases of the common cold (which is also caused by other viruses, predominantly rhinoviruses), while more lethal varieties can cause SARS, MERS, and COVID-19. In cows and pigs they cause diarrhea, while in mice they cause hepatitis and encephalomyelitis. There are as yet no vaccines or antiviral drugs to prevent or treat human coronavirus infections.
Coronaviruses constitute the subfamily Orthocoronavirinae, in the family Coronaviridae, order Nidovirales, and realm Riboviria.[5][4] They are enveloped viruses with a positive-sense single-stranded RNA genome and a nucleocapsid of helical symmetry. The genome size of coronaviruses ranges from approximately 26 to 32 kilobases, one of the largest among RNA viruses. They have characteristic club-shaped spikes that project from their surface, which in electron micrographs create an image reminiscent of the solar corona, from which their name derives.
The question is how to end this pandemic with herd immunity. There is enough anecdotal data to say that immunity with COVID-19 is short-lived, letting the illness just run its course will not achieve herd immunity as immunity wears off. “Science” is looking to immunization to create this immunity.
In controlling the spread of a disease, the level of the population which needs to be immune will vary by the contagiousness of the disease. Note that COVID-19 is migrating from more deadly / less contagious to less deadly / more contagious form. In theory, a pandemic dies out if one person with COVID-19 infects less than one person on average.
Note that “science” has yet to field a truly effective vaccine against any coronavirus – or even the simple flu. According to the CDC:
CDC conducts studies each year to determine how well the influenza (flu) vaccine protects against flu illness. While vaccine effectiveness (VE) can vary, recent studies show that flu vaccination reduces the risk of flu illness by between 40% and 60% among the overall population during seasons when most circulating flu viruses are well-matched to the flu vaccine. In general, current flu vaccines tend to work better against influenza B and influenza A(H1N1) viruses and offer lower protection against influenza A(H3N2) viruses.
[editor’s note: the flu vaccination does not reduce hospitalizations, death in older adults]
The health care professionals and the NIH / CDC have long been dropping hints that they do not expect 100 % efficacy [efficacy is measured by comparing the rate of illness in the vaccinated and the placebo groups]. For herd immunity to be achievable, nearly the entire population needs to be immunized if efficacy is barely above 50%.
The current COVID-19 immunization trials will only answer two important questions:
- that the vaccine will have little adverse effects
- that the vaccine reduces the spread of COVID-19
The current COVID-19 immunization trials will not answer:
- that the immunization will reduce the hospitalization rate
- that the immunization will reduce the death rate
- the length of time the vaccine creates immunity
The unanswered questions will be answered months and years after the vaccine is first approved and released for use to the general population. Yes, the general population will be the guinea pigs for this research. Note that I am not suggesting there is a better way to roll out the vaccine as the world cannot wait for the answers. And the first vaccine approved may not be the most effective. But this does explain why many people are reluctant to be immunized at the time the first vaccine is approved – they do not want to be guinea pigs.
Is there light at the end tunnel? – Yes, but it may not be bright enough.
Coronavirus News You May Have Missed
Wanted: Online gamers to help build a more stable Covid-19 vaccine – Knowable
Quickly vaccinating billions of people around the globe against Covid-19 is going to be an endeavor like no other in human history. What could make it even more difficult is that some of the leading contenders — mRNA vaccines — have a very short shelf life: They have to be stored and shipped at temperatures as low as minus 80 degrees Celsius (minus 112 degrees Fahrenheit).
The private sector, as well as the US military, is trying to figure out how to manage that feat. But there’s another possibility — and it relies on thousands of people playing an online game.
A relatively new technology, mRNA vaccines are promising because they can be created and manufactured quickly. Pfizer and Moderna’s vaccine candidates (two of the first three to begin Phase 3 clinical trials in the United States) are mRNA vaccines. Once thawed, however, an mRNA vaccine has to be used immediately. Without a breakthrough, such vaccines wouldn’t be available at local pharmacies, community centers or libraries, as the flu shot is. They probably would never reach developing countries.
… So why tackle this scientific inquiry with a game? It turns out that big groups of humans are better — significantly so — at coming up with brand-new RNA structures than even the latest kinds of artificial intelligence. (Read more about scientific discovery through games in the 2019 Annual Review of Biomedical Data Science.)
No one knows exactly why this is. It seems to be, in part, because AI has baseline parameters set by only a few humans, while the game leverages the knowledge of thousands — programmers and plumbers, architects and astrophysicists, gamers and grandparents.
These diverse individuals take on weekly Eterna challenges that are created in a collaboration between Stanford scientists and dozens of committed players. Given the vast structural possibilities, players routinely generate RNA molecules that look like flowers, beaded necklaces, antlers and other shapes never seen before by RNA researchers.
That’s why Eterna needs to recruit thousands more players. More players, more new designs. Also, more players equals greater collective wisdom on winnowing the options down to the most promising mRNA designs, which are then synthesized in a university lab and examined to check their longevity (and to be sure they still create the correct protein to spur an immune response). With guidance from the most dedicated, experienced players, scientists use these lab results to create the next set of hypotheses to be tested with Eterna puzzles.
Musicians Improvise Masks for Wind Instruments to Keep the Band Together – Kaiser Health
Trombonist Jerrell Charleston loves the give-and-take of jazz, the creativity of riffing off other musicians. But as he looked toward his sophomore year at Indiana University, he feared that steps to avoid sharing the coronavirus would also keep students from sharing songs.
… His worries evaporated when he arrived on campus and discovered that music professor Tom Walsh had invented a special mask with a hole and a protective flap to allow musicians to play while masked.
Students also got masks for the ends of their wind instruments, known as bell covers, allowing them to jam in person, albeit 6 feet apart.

Home tests could help in the fight against the coronavirus. So where are they? – Washington Post
Ten months into the coronavirus pandemic, the promise of a rapid and inexpensive at-home test for the virus remains unfulfilled as companies struggle to overcome final regulatory hurdles.
The technology for such tests exists, and early versions are being used in nursing homes and schools. But companies racing to bring the tests to the wider U.S. market must make them more accurate and easier to use before they can meet federal guidelines that would allow sales directly to consumers.
Although no single test will end the pandemic in the United States, experts say the ability for people to take a test at home and know within minutes whether they’re infected could be an important component in stanching the spread of the virus.
Such a test could be taken several days ahead of a visit with grandparents, for example. Or before heading into work. And if a local outbreak occurs, officials could hand out hundreds of at-home rapid tests to find and stop viral transmission.
… Some retailers, including Costco, have begun selling home tests to consumers, but they are costly — about $130 — and require people to mail their sample to a lab and wait 24 to 48 hours for results. The rapid tests now being developed could cost as little as $5 and take 15 minutes for results.
At least two dozen companies are trying to develop home tests, most of them antigen tests that detect proteins on the surface of the virus. Some companies are tantalizingly close to clearing final barriers.
In July, the Food and Drug Administration issued guidelines making clear that any home test needs to be accurate and easy enough for untrained people to use without confusion.
Since then, the agency has not received any applications from companies for home tests, the agency said.
[editor’s note: this post deserves a full read]
Coronavirus tests performed in labs are the gold standard for accuracy and antigen tests are a fast and inexpensive alternative.
But backers of a third type of test, developed by a Nobel Prize winner using cutting-edge CRISPR technology, say it has the potential to be all three: rapid, accurate and inexpensive.
Although these gene-editing technology tests are still being developed and won’t be ready in the United States this year as the weather cools and demand surges, research groups recently published scientific papers describing them as an appealing alternative as testing shortages persist in the COVID-19 pandemic.
Dr. Jennifer Doudna, a University of California, Berkeley researcher whose pioneering work in CRISPR earned a share of this year’s Nobel Prize in chemistry, said the test can be done quickly and doesn’t require a lab.
“We have a ways to go before CRISPR-based diagnostics reach widespread use, but I believe we’ll see an impact during the current pandemic,” Doudna said. “Because it is simple to adjust these tests to detect other targets, the platform we’re developing now is laying the groundwork to deploy CRISPR for rapid diagnosis during future outbreaks.”
[editor’s note: this post is worth a full read]
Universal Mask Wearing Could Save Some 130,000 Lives In The U.S., Study Suggests – NPR
Universal mask wearing in public could greatly reduce the number of Americans who die by COVID-19 by February, a study published Friday in the journal Nature Medicine projects.
Researchers at the University of Washington’s Institute for Health Metrics and Evaluation made estimates based on some assumptions under different scenarios.
In what they describe as the worst-case scenario, they project that COVID-19 deaths could exceed a million between September 2020 and February 2021 if what they call “the current pattern of easing” restrictions continues in states.
In a second scenario that they think is more likely, they say 511,000 could die between September and February under the assumption that “states would once again shut down social interaction and some economic activity” for six weeks once deaths reach a certain threshold per million residents.
But in a third scenario where 95% of the population dons face coverings and social restrictions are in place, the projection is for deaths to be about 381,000 — or about 130,000 fewer than under the second scenario.
If that mask percentage changes to 85% of Americans with restrictions, it could still save some 96,000 lives, they say.
In coronavirus testing, false positives are more hazardous than they might seem. – New York Times
In the high-stakes world of coronavirus testing, false positives are widely considered to be benign in comparison with false negatives, which can deprive infected people of treatment and embolden them to mingle with others, hastening the spread of disease.
But false positives, which incorrectly identify a healthy person as infected by the virus, can have serious consequences as well, especially in places where the virus is scarce.
False positives are generally very rare among tests that have been vetted by the Food and Drug Administration. But any test can be plagued by contamination, mishandling or technical glitches, leading a device to spot the coronavirus where it is not.
In places where the virus is relatively scarce, false positives may even outnumber accurate positives — eroding trust in tests and, under some circumstances, prompting outbreaks of their own.
Adverse effects include:
- Unnecessary isolation
- New outbreaks
- Missed or inappropriate treatment
- A false sense of security
The following are foreign headlines with hyperlinks to the posts
‘Soon the Dead Will Start Arriving Again,’ Italian Cemetery Worker Says
As the pandemic cripples Airbnb, European cities see a chance to reclaim long-term housing.
Italy closes gyms and theaters to fight a steep rise in coronavirus infections.
The following are additional national and state headlines with hyperlinks to the posts
As COVID-19 forces them to slow down, families find joy in spending more time together
How California turned the corner on COVID-19
Two Loeffler staffers test positive for COVID-19
Record numbers of daily infections are reported in six states, including Ohio and Illinois.
Will masks become the ‘new normal’ even after the pandemic has passed? Some Americans say so
White House chief of staff: ‘We are not going to control the pandemic’
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
Coronavirus Disease Weekly News 24October 2020
Coronavirus Economic Weekly News 24October 2020
How Does The Pandemic Recession Stack Up Against The Great Depression?
Energy Sector Slow To Recover From Malaise Arising From Effects Of Global Pandemic
How Do Consumers Believe The Pandemic Will Affect The Economy And Their Households?
Infographic Of The Day: Mask Waste Is Hurting The Planet And You Too
New Understanding Of Neuropilin-1 Protein Could Speed Vaccine Research
Warning to Readers
The amount of politically biased articles on the internet continues to increase. And studies and opinions of the experts continue to contradict other studies and expert opinions. Honestly, it is difficult to believe anything anymore. A study usually cannot establish cause and effect – but only correlation. Be very careful what you believe about this pandemic.

I assemble this coronavirus update daily – sifting through the posts on the internet. I try to avoid politically slanted posts (mostly from CNN, New York Times, and the Washington Post) and can usually find unslanted posts on that subject from other sources on the internet. I wait to publish posts on subjects that I cannot validate across several sources. But after all this extra work, I do not know if I have conveyed the REAL facts. It is my job to provide information so that you have the facts necessary – and then it is up to readers to draw conclusions.
Coronavirus INTERACTIVE Charts
include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus.htm’); ?>
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19. At this point, herd immunity does not look like an option although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a higher death rate.
- There are at least 8 strains of the coronavirus. New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
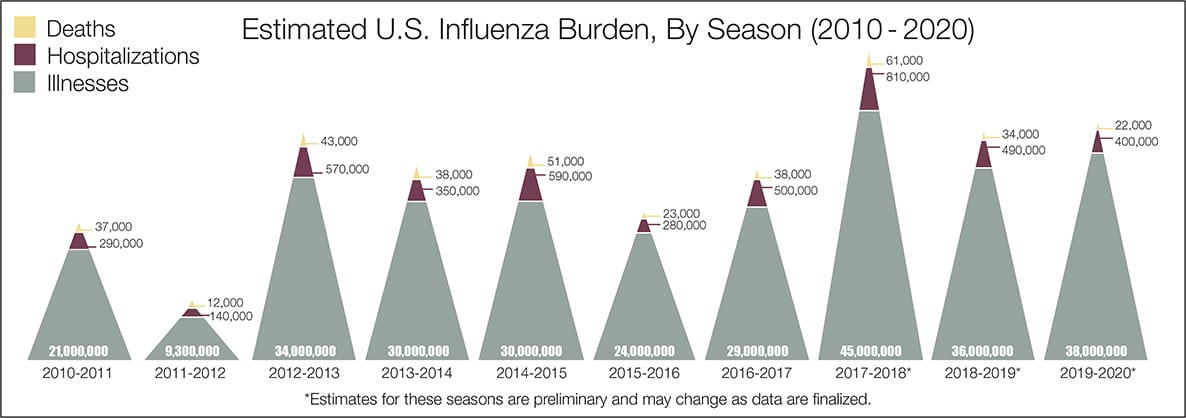
- The real question remains if the U.S. is over-reacting to this virus. The following graphic from the CDC puts the annual flu burden in perspective [click on image to enlarge]. Note that using this data is dangerous as the actual flu cases are estimated and not counted – nobody knows how accurate these guesses are.
What we do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work.
- Do we develop lasting immunity to the coronavirus? Another coronavirus – the simple cold – does not develop long term immunity.
- To what degree do people who never develop symptoms contribute to transmission?
- The US has scaled up coronavirus testing – and the accuracy of the tests has been improving. However, if one loses immunity – the coronavirus testing value is reduced.
- Can children widely spread coronavirus? [current thinking is that they are becoming a major source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- What effect will the weather have? At this point, it does not seem hot weather slows this coronavirus down – and it seems air conditioning contributes to its spread.
- Outdoor activities seem to be a lower risk than indoor activities.
- Can the world really push out an effective vaccine in 12 to 18 months?
- Will other medical treatments for Covid-19 ease symptoms and reduce deaths? So far only one drug (remdesivir) is approved for treatment.
- A current scientific understanding of the way the coronavirus works can be found [here].
Heavy breakouts of coronavirus have hit farm workers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of the respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>





