Written by Steven Hansen
The U.S. new cases 7-day rolling average are 58.0 % HIGHER than the 7-day rolling average one week ago and U.S. deaths due to coronavirus are now 27.4 % HIGHER than the rolling average one week ago.
Today’s posts include:
- U.S. Coronavirus New Cases are 95,083
- U.S. Coronavirus deaths are at 386
- New details on CDC’s Provincetown investigation portray delta variant as serious threat
- Leaked CDC Report Claims Delta Spreads As Easily As “Chickenpox”
- ‘The war has changed’: Internal CDC document urges new messaging, warns delta infections likely more severe
- Delta variant: The epidemic will sweep across the U.S. at different times, Dr. Scott Gottlieb says
- Iceland’s Chief Epidemiologist Suggests COVID-19 Restrictions Could Last For Up To 15 Years
- Covid is more mysterious than we often admit
- Lambda Variant of COVID-19 Might Be Resistant to Vaccines
- Biden push to vaccinate feds forces uncomfortable questions
- All Vaxxed Up and Nowhere to Go
- Call in the T-Cell Cavalry to Fight COVID in the Immunocompromised
- Strong, but disappointing, U.S. GDP report may be bad news for the Fed
- Plus many more headlines …

include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus1.htm’); ?>
Hospitalizations Are The Only Accurate Gauge
Hospitalizations historically appear to be little affected by weekends or holidays. The hospitalization growth rate trend continues to improve.

source: https://gis.cdc.gov/grasp/covidnet/COVID19_3.html
Historically, hospitalization growth follows new case growth by one to two weeks.
As an analyst, I use the rate of growth to determine the trend. But, the size of the pandemic is growing in terms of real numbers – and if the rate of growth does not become negative – the pandemic will overwhelm all resources.
The graph below shows the rate of growth relative to the growth a week earlier updated through today [note that negative numbers mean the rolling averages are LOWER than the rolling averages one week ago]. As one can see, the rate of growth for new cases peaked in early December 2020 for Thanksgiving, and early January 2021 for end-of-year holidays – and it now shows that the coronavirus effect is improving.

In the scheme of things, new cases decline first, followed by hospitalizations, and then deaths. The potential fourth wave did not materialize likely due to immunizations.
Coronavirus and Recovery News You May Have Missed
Iceland’s Chief Epidemiologist Suggests COVID-19 Restrictions Could Last For Up To 15 Years – ZeroHedge
Iceland’s chief epidemiologist has suggested that some COVID-19 lockdown restrictions may remain in place for as long as fifteen years.
Þórólfur Guðnason, a doctor who serves as the Chief Epidemiologist of the Icelandic Directorate of Health, was quizzed by journalist Esther Hallsdóttir how long the rules should continue.
Guðnason was, “Asked if there is no clear way out of the epidemic, now that measures are being proposed despite vaccinations, and whether we could be on the verge of restrictions over the next five, ten or fifteen years.”
His response was in the affirmative.
“It can be quite like that, no one can say with certainty what the future will be like. That’s what we’re always been saying, too, that there’s no predictability in this,” said Guðnason.
“It is nothing new and many people complain that it is not possible to bring predictability in operations and such, but it is not possible when the virus is unpredictable and something new comes up that changes what you thought a few months ago,” he added.
As we previously highlighted, SAGE government advisor and proud Communist Party member Susan Michie went even further, asserting that things like social distancing and mask mandates should last “forever.”
Another doctor in the UK who wants lockdown to remain in place indefinitely lamented that, “sadly, it can’t be forever.”
As we highlighted earlier this month, British author Peter Hitchens warned that if people continued to blithely accept lockdown restrictions, their grandchildren will still be wearing masks in 2050 and no one will remember why.
Covid is more mysterious than we often admit. – New York Times
Consider these Covid-19 mysteries:
- In India — where the Delta variant was first identified and caused a huge outbreak — cases have plunged over the past two months. A similar drop may now be underway in Britain. There is no clear explanation for these declines.
- In the U.S., cases started falling rapidly in early January. The decline began before vaccination was widespread and did not follow any evident changes in Americans’ Covid attitudes.
- In March and April, the Alpha variant helped cause a sharp rise in cases in the upper Midwest and Canada. That outbreak seemed poised to spread to the rest of North America — but did not.
- This spring, caseloads were not consistently higher in parts of the U.S. that had relaxed masking and social distancing measures (like Florida and Texas) than in regions that remained vigilant.
- Large parts of Africa and Asia still have not experienced outbreaks as big as those in Europe, North America and South America.
- How do we solve these mysteries? Michael Osterholm, who runs an infectious disease research center at the University of Minnesota, suggests that people keep in mind one overriding idea: humility.
“We’ve ascribed far too much human authority over the virus,” he told me.
‘Much, much milder’
Over the course of this pandemic, I have found one of my early assumptions especially hard to shake. It’s one that many other people seem to share — namely, that a virus always keeps spreading, eventually infecting almost the entire population, unless human beings take actions to stop it. And this idea does have crucial aspects of truth. Social distancing and especially vaccination can save lives.But much of the ebb and flow of a pandemic cannot be explained by changes in human behavior. That was true with influenza a century ago, and it is true with Covid now. An outbreak often fizzles mysteriously, like a forest fire that fails to jump from one patch of trees to another.
The experience with Alpha in the Midwest this spring is telling:
Even Osterholm said that he had assumed the spring surge would spread from Michigan and his home state of Minnesota to the entire U.S. It did not. It barely spread to nearby Iowa and Ohio. Whatever the reasons, the pattern shows that the mental model many of us have — in which only human intervention can have a major effect on caseloads — is wrong.Britain has become another example. The Delta variant is even more contagious than Alpha, and it seemed as though it might infect every unvaccinated British resident after it began spreading in May. Some experts predicted that the number of daily cases would hit 200,000, more than three times the country’s previous peak. Instead, cases peaked — for now — around 47,000, before falling below 30,000 this week.
“The current Delta wave in the U.K. is turning out to be much, much milder than we anticipated,” wrote David Mackie, J.P. Morgan’s chief European economist.
True, you can find plenty of supposed explanations, including the end of the European soccer tournament, the timing of school vacations and the Britain’s notoriously late-arriving summer weather, as Mark Landler, The Times’s London bureau chief, has noted. But none of the explanations seem nearly big enough to explain the decline, especially when you consider that India has also experienced a boom and bust in caseloads. India, of course, did not play in Europe’s soccer championship and is not known for cool June weather.‘Rip through’
A more plausible explanation appears to be that Delta spreads very quickly at first and, for some unknown set of reasons, peters out long before a society has reached herd immunity. As Andy Slavitt, a former Covid adviser to President Biden, told me, “It seems to rip through really fast and infect the people it’s going to infect.” The most counterintuitive idea here is that an outbreak can fade even though many people remain vulnerable to Covid.
That’s not guaranteed to happen everywhere, and there probably will be more variants after Delta. Remember: Covid behaves in mysterious ways. But Americans should not assume that Delta is destined to cause months of rising caseloads. Nor should they assume that a sudden decline, if one starts this summer, fits a tidy narrative that attributes the turnaround to rising vaccination and mask wearing.
“These surges have little to do with what humans do,” Osterholm argues. “Only recently, with vaccines, have we begun to have a real impact.”


Biden push to vaccinate feds forces uncomfortable questions – AP
President Joe Biden’s requirement for federal workers to reveal their COVID-19 vaccination status is likely to force uncomfortable questions not only at government agencies but at private companies as well.
Right now, there’s a lack of clear answers.
Getting the policy right will take time, and vary across government agencies. The same holds for private companies, for which the White House is trying to provide a guide. It’s not like there’s a cheat sheet. Nothing on this scale has been attempted before in the face of a virus morphing in real time to become a bigger threat.
“We developed a miracle vaccine in a very short period of time, and there has been a lot hesitancy from the government and from businesses to run with a top-down approach,” said Andrew Challenger, senior vice president at the workforce consulting firm Challenger, Gray & Christmas. “Now we’ve reached a point where it’s become very clear the individual incentive people have to protect themselves has not been strong enough to protect the country, and we’re seeing the government take this first step.”
Instead, workers will have to attest to whether they’re vaccinated. Although employees will not be required to produce a vaccination card, “attest” is a loaded word in the federal workplace, minutely governed by rules and regulations. It implies consequences for providing false or misleading information. How that will be enforced remains unclear, but employees who voluntarily provide valid proof of vaccination will likely settle potential questions upfront.
The unvaccinated will have to put up with regular testing, required masking and social distancing, and they will be barred from official travel. Similar rules will be applied to federal contractors.
Continual testing raises other issues. For most people, health insurance has been paying. But will that continue if someone refuses to be vaccinated and is not eligible for medical or religious exemptions?
Masking has been a perennially touchy subject. But how will agencies enforce a masking policy if not everyone is required to be vaccinated? Will supervisors patrol the cubicles with lists of the unvaccinated?
There are many reasons why translating Biden’s order to the workplace may not go smoothly. Government agencies tend to have their own unique cultures, and their missions run the gamut. Doctors at the National Institutes of Health are probably already vaccinated, but some law enforcement agents may be wary of getting a shot not yet fully approved by the Food and Drug Administration.
[editor’s note: also read Biden Mandates All Federal Workers Must Be Vaccinated… Except Postal Workers]
All Vaxxed Up and Nowhere to Go – MedPage
As tens of thousands of Americans — myself included — have discovered, getting a pair of COVID-19 vaccination shots isn’t an instant all-access ticket to pandemic freedom. We’re stuck in limbo because we participated in clinical trials of vaccines that haven’t yet been authorized for use in the U.S.
Computer systems, foreign nations, universities, and a cruise line refuse to believe we’ve been vaccinated. We’re facing workplace hassles, worrying about international travel, and wondering if we can attend sports events, conferences, and performances. Some of us have even gotten re-vaccinated with authorized vaccines even though no one knows if double-dipping is a good idea.
“The whole thing is a ridiculous mess,” virologist John P. Moore, PhD, of Weill Cornell Medicine in New York City, told MedPage Today. “Trial participants can really be in a gray area — an intersection between bureaucracy and the real world.”
Like 30,000 others in the U.S. and Mexico, Moore was a participant in a Novavax COVID-19 vaccine trial and received a pair of injections earlier this year, along with two doses of a placebo. The company has touted study results that seem impressive. But its vaccine is not yet authorized for use anywhere in the world, and it does not appear on the World Health Organization’s (WHO) influential list of COVID-19 vaccines authorized for emergency use.
The 30,000-plus U.S. participants in an AstraZeneca trial are in a similar pickle. Their vaccine is not authorized in the U.S., although it is reportedly authorized in 119 countries and by the WHO.
Both Novavax and AstraZeneca have begun distributing vaccine cards — they’re specially modified in Novavax’s case — but it remains to be seen if governments, workplaces, and venues will accept them as proof of vaccination. Meanwhile, vaccination requirements for health workers and others are rapidly becoming more common across the country.
No one seemed to have anticipated travel and workplace hassles when Novavax began recruiting for vaccine trials in the second half of 2020. The 31-page consent form I signed in January to take part in the Novavax trial said nothing about the prospect that much of the world would consider my study vaccination to be invalid. Yet that’s exactly what happened, sparking a bitter backlash on social media.
Delta variant: The epidemic will sweep across the U.S. at different times, Dr. Scott Gottlieb says – CNBC
- Dr. Scott Gottlieb told CNBC on Wednesday he believes U.S. could see downslope from delta Covid surges in two to three weeks.
- Gottlieb did warn, however, that northern states may start to see more delta spread, as rates decrease in the south.
Strong, but disappointing, U.S. GDP report may be bad news for the Fed – MarketWatch
Thursday’s strong, but disappointing, U.S. second-quarter GDP figure may be something of a warning flag for Federal Reserve officials.
There’s a risk that economic growth going forward could come in below forecasters’ estimates, leaving the U.S. mired in a slower-than-anticipated growth pattern for 2022 and possibly 2023 after a sharp, but short, recovery from the Covid-19 crisis, says Eric Vanraes, a Geneva, Switzerland-based bond portfolio manager at Eric Sturdza Investments, which managed $2.9 billion as of June.
And that’s bad news for the Federal Reserve because policy makers may have already missed the “sweet spot” for pivoting toward a more hawkish policy stance, Vanraes said via phone Thursday. At the conclusion of a two-day meeting yesterday, central bankers indicated they would use coming meetings to assess whether enough progress has been made to start tapering their $120 billion in monthly bond purchases — suggesting the process could get underway later this year.
“The problem is that, even before the Covid crisis, we were anticipating a U.S. slowdown in 2022,” Vanraes said. “Now we have had a relatively sharp recovery, followed by a less-than-sharp GDP number today. We do not exclude a slowdown in one year or 18 months from now and if there is one, it will be very difficult for the Fed to become more hawkish when it needs to. So it’s a bit complicated.”
Vanraes isn’t alone. Dan Eye, head of asset allocation and equity research at Fort Pitt Capital Group based in Pittsburgh, says the biggest risk in financial markets right now is that “valuations are high, with the S&P 500 index trading at 21.3 times earnings, along with very aggressive positioning, and there’s not much of cushion out there for any type of unexpected outcomes.”
‘The war has changed’: Internal CDC document urges new messaging, warns delta infections likely more severe – Washington Post
The delta variant of the coronavirus appears to cause more severe illness than earlier variants and spreads as easily as chickenpox, according to an internal federal health document that argues officials must “acknowledge the war has changed.”
The document is an internal Centers for Disease Control and Prevention slide presentation, shared within the CDC and obtained by The Washington Post. It captures the struggle of the nation’s top public health agency to persuade the public to embrace vaccination and prevention measures, including mask-wearing, as cases surge across the United States and new research suggests vaccinated people can spread the virus.
The document strikes an urgent note, revealing the agency knows it must revamp its public messaging to emphasize vaccination as the best defense against a variant so contagious that it acts almost like a different novel virus, leaping from target to target more swiftly than Ebola or the common cold.
It cites a combination of recently obtained, still-unpublished data from outbreak investigations and outside studies showing that vaccinated individuals infected with delta may be able to transmit the virus as easily as those who are unvaccinated. Vaccinated people infected with delta have measurable viral loads similar to those who are unvaccinated and infected with the variant.
“I finished reading it significantly more concerned than when I began,” Robert Wachter, chairman of the Department of Medicine at the University of California at San Francisco, wrote in an email.
CDC scientists were so alarmed by the new research that the agency earlier this week significantly changed guidance for vaccinated people even before making new data public.
The data and studies cited in the document played a key role in revamped recommendations that call for everyone — vaccinated or not — to wear masks indoors in public settings in certain circumstances, a federal health official said. That official told The Post that the data will be published in full on Friday. CDC Director Rochelle Walensky privately briefed members of Congress on Thursday, drawing on much of the material in the document.
[editor’s note: I would read the next post from ZeroHedge which puts this into perspective]
“The War Has Changed” – Leaked CDC Report Claims Delta Spreads As Easily As “Chickenpox” – ZeroHedge
The CDC is clearly concerned that it’s losing the PR war to convince Americans that they must mask up and get vaccinated. Because less than a week after declaring that it would revive its mask mandate, the CDC has just pulled a classic media trick: turning the fearmongering nob up to ’11’ by leaking an “internal report” that supports the official narrative (even making it look like the more moderate of two options) while laundering the source of the information by allowing a reputable news org to market the story as an “exclusive”.
A slide deck apparently shared widely inside the agency in the weeks after it first lifted the original mask mandate in May shows that the delta variant appears to cause more severe illness in younger patients, while spreading as easily as “chickenpox.” What’s more, it warns that the vaccine’s ability to spread via infecting the already vaccinated means the CDC should impose even more stringent guidance – the presentation called for “universal masking.” The document “strikes an urgent note, revealing the agency knows it must revamp its public message to emphasize vaccination as the best defense against a variant so contagious that it acts almost like a different novel virus.”
Most critically, the slide deck includes “still-unpublished data” from studies showing that even the vaccinated might be able to transmit the virus as easily as the unvaccinated.
According to the Washington Post, the material in the report was “so alarming” that it prompted the CDC to reconsider its masking guidance, and President Biden to impose his federal employee vaccination mandate (with a few notable exceptions) despite his earlier promises not to do so.
Not only does the presentation include “new science”, it also suggests “a new strategy” for communicating the urgency of the situation to the public, noting that “public trust in vaccines might be undermined” when people hear about breakthrough infections. At one point, the deck declared that “the war has changed,” describing delta as if it were a totally new virus.
Well, maybe Pfizer and the government should have thought about that before they published obviously inflated efficacy numbers of +90%.
Despite that obvious blunder, WaPo was still able to fund a talking head to praise the government’s vaccine strategy.
Matthew Seeger, a risk communication expert at Wayne State University in Detroit, said a lack of communication about breakthrough infections has proved problematic. Because public health officials had emphasized the great efficacy of the vaccines, the realization that they aren’t perfect may feel like a betrayal.
“We’ve done a great job of telling the public these are miracle vaccines,” Seeger said. “We have probably fallen a little into the trap of over-reassurance, which is one of the challenges of any crisis communication circumstance.”
Data showing the vaccines aren’t as effective against the variants isn’t exactly groundbreaking. We’ve seen similar reports from other sources, notably the Israeli Health Ministry.
The thing to remember here is that this data is already dated. The story readily admits the presentation was circulated months ago.
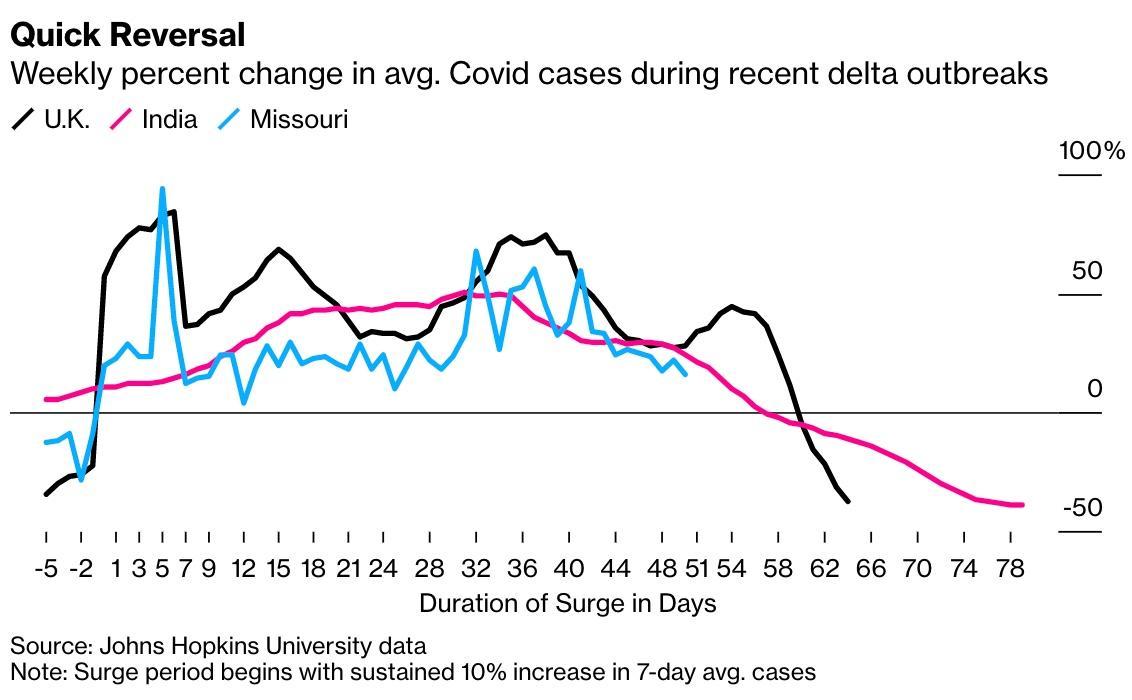
Former FDA head Dr. Scott Gottlieb has highlighted data suggesting that the US outbreak will follow a similar trajectory as delta-driven outbreaks in the UK and Europe. The pattern is already most obvious in states like Missouri, one of the original hotbeds for the delta outbreak.
The key to understanding this is a rate known as Rt, a representation of how many people are being infected by each new case. When it falls below 1, that means the rate of viral spread is slowing. And the data suggest that it’s already on that trajectory.
[editor’s note: look at the next ABC post which is even more concerning]
New details on CDC’s Provincetown investigation portray delta variant as serious threat – ABC
Adding more insight into the CDC’s updated mask guidance, newly published details of the Provincetown outbreak raise concern that the now-dominant delta variant may be able to spread among fully vaccinated people.
Following multiple large gatherings in Provincetown, Mass., from July 3-17, investigators identified 469 COVID-19 cases, two-thirds of which were in fully vaccinated people. The delta variant was responsible for 90% of those cases. The breakthrough infections were among people vaccinated with Pfizer, Moderna and Johnson & Johnson. None of the vaccinated people died, but most had some symptoms.
During the outbreak investigation, researchers learned that the amount of virus in the noses of vaccinated people experiencing a breakthrough infection was the same as in an unvaccinated person — a worrying sign that vaccinated people can spread the virus.
“This finding is concerning and was a pivotal discovery leading to CDC’s updated mask recommendation,” said CDC Director Rochelle Walensky in a statement.
“This is a very concerning outbreak — pretty much a ‘super spreader event,'” said Dr. Carlos Del Rio, executive associate dean and global health expert at the Emory School of Medicine.
CDC Alarmed: 74% of Cases in Cape Cod Cluster Were Among the Vaxxed – MedPage
Breakthrough infections were responsible for three-quarters of COVID-19 cases in an outbreak during large public gatherings on Cape Cod, Massachusetts, and nearly all sequenced cases were the Delta variant, researchers found.
Of 469 cases linked to multiple summer events and large summer gatherings in a small town, 346 (74%) occurred in fully vaccinated people, and almost 80% of those cases were symptomatic, reported Catherine Brown, DVM, of the Massachusetts Department of Public Health, and colleagues.
There were five hospitalizations, four among fully vaccinated people, and no deaths. Of 133 cases with sequence information available, 89% were from the Delta variant (B.1.617.2), the authors wrote in an early edition of the Morbidity and Mortality Weekly Report.
Moreover, vaccination coverage in Massachusetts was reported to be 69% as of July 3, they noted.
Topline data were previewed in stories by the New York Times on Thursday, and shared in internal CDC documents by the Washington Post. The data on this outbreak, and the Delta variant, reportedly helped provide the impetus for the agency’s change in indoor masking guidance earlier this week. While the town was not named by the MMWR report, the outbreak reportedly was linked to events in Provincetown.
Lambda Variant of COVID-19 Might Be Resistant to Vaccines – Infection Control Today
Investigators in Chile conclude that the lambda COVID-19 variant is not only more infectious than standard SARS-CoV-2, but could also possibly shrug off vaccines. The first case in the United States has been spotted at Houston Methodist Hospital.
A COVID-19 variant that proves to be resistant to vaccines keeps medical experts, public health officials, and health care professionals—including infection preventionists—on the frontlines of the COVID-19 pandemic up at nights. There’s no reason to sound the alarm yet, but there may—just may—perhaps be reason to think that there’s a chance that the alarm may have to be sounded at some point about the lambda COVID-19 mutation, or C.37.
A preprint study by investigators in Chile suggests that the mutation, which first surfaced in Peru about a year ago and is highly infectious, may also be able to evade vaccine antibodies.
“Our results indicate that mutations present in the spike protein of the lambda variant of interest confer increased infectivity and immune escape from neutralizing antibodies elicited by CoronaVac,” the study states. CoronaVac is a vaccine manufactured by a Chinese company and that’s used in Peru. The study continues: “These data reinforce the idea that massive vaccination campaigns in countries with high SARS-CoV-2 circulation must be accompanied by strict genomic surveillance allowing the identification of new isolates carrying spike mutations and immunology studies aimed to determine the impact of these mutations in immune escape and vaccines breakthrough.”
Peru has the highest COVID-19 death rate of any country in the world, according to the Johns Hopkins Coronavirus Resource Center: about 600 for every 100,000 people infected with COVID-19. That’s about twice the amount of Hungary, the country with the next highest COVID-19 death rate. The World Health Organization (WHO) says that the lambda variant has been the COVID carrier in about 81% of infections in Peru since April. The WHO declared the lambda variant a variant of interest last month. The lambda variant has spread to about 30 other countries in the world, including the United Kingdom.
The first case of lambda variant has been spotted at Houston Methodist Hospital about 2 days ago, according various news outlets, including Axios. An ironic development, as Houston Methodist Hospital has sparked headlines lately by being the first hospital in the U.S. to mandate that all its employees get the COVID-19 vaccine. As Infection Control Today® reported, 153 of Houston Methodist Hospital’s employees either resigned or were fired for not getting the vaccine. KHOU 11 reports that there’s been an alarming spike in COVID-19 infections in the Houston area. Houston Methodist Hospital officials have not commented on whether the loss of those 153 employees has hindered the facility’s ability to treat the influx of patients.
Call in the T-Cell Cavalry to Fight COVID in the Immunocompromised – MedPage
Last year was one of collective confinement. The majority of us shuttered our doors to visitors, worked from home, and ventured out sparingly in hopes of evading the grasp of COVID-19. Now in 2021, thanks to vaccination rollout, those who have been vaccinated are hopefully on the path to normalcy. But not everyone is so fortunate. For some, 2021 will bring more isolation and loneliness than ever before, which is hard to imagine. I’m talking about immunocompromised adults and children. While much of the rest of the populace clinks glasses, hugs loved ones, and joins parties, immunocompromised individuals do not have the security of an effective vaccine, and for their health and safety will maintain their distance and watch the social revelry from the sidelines.
The normal vaccine response that elicits antibodies and immune cells to fight infection are absent in these immunocompromised individuals, who fall into two categories: those living with congenital or acquired diseases that weaken their immune system, or those with pre-existing conditions whose treatment requires dampening of the immune system (e.g., patients with blood cancers or transplant recipients). This vulnerable population represents a sizable proportion of the U.S. population. A 2018-2019 analysis in JAMA Network Open estimated that 2.8% of adults in America were on a treatment regimen that dampened their immune system. That percentage may seem small but extrapolate it to the entire U.S. population and you hit 9 million vulnerable people. This doesn’t even include immunocompromised individuals who are not taking immune-suppressing medication.
The plight of immune-compromised individuals has large-scale implications. This inability to combat the virus not only can be potentially life-threatening but can also lead to the continued evolution of mutant strains that infiltrate healthy populations. The so-called New York variant (B.1.526) was identified in a patient with advanced AIDS. Similarly, the highly transmissible and more deadly Alpha strain (B.1.1.7) emerged in a patient receiving immune suppressive treatment for a blood cancer.
So, while COVID-19 vaccines administered in the U.S. have been highly effective for mounting an antibody immune response in people with functional immune systems, it’s not enough to vanquish the contagion. In our fight against virus infection, another critical arm of the immune system is required: The T-cell immune response. While antibodies may prevent infection, these warriors destroy already infected cells. And initial research suggests they may be active even in absence of antibodies.
Just recently, researchers (including myself) published a study in the Journal of Clinical Immunology that showed that pediatric patients with primary immune deficiencies, who often fail to make protective immune responses to infections and vaccinations, show robust T-cell activity and immunity against SARS-CoV-2. These findings are important because if T-cell responses to COVID-19 are protective in this highly vulnerable population, this could suggest that a COVID-19-directed T-cell immunotherapy might benefit other profoundly immunocompromised patients. However, we still don’t know if such responses will persist to provide protective long-term immunity, especially against mutant strains of the virus.
The following are foreign headlines with hyperlinks to the posts
The following additional national and state headlines with hyperlinks to the posts
Pentagon says it will start talks on making COVID-19 vaccine mandatory
Biden called on states and localities to use federal money to pay unvaccinated people $100 to get a shot.
The Pentagon said vaccine requirements for federal workers would apply to active-duty military.
The Delta variant is as contagious as chickenpox, an internal C.D.C. document says.
The E.U. has a higher vaccination rate than the U.S., as these charts show.
hospitalizations are threefold higher in states where the fully vaccinated rate remains stuck below 50%.
According to the latest CDC numbers, two-thirds of the vaccine-eligible U.S. population (ages 12 and up) have received at least one shot, with 57.7% now fully vaccinated.
White-tailed deer — part of the cervid family — are just like us, at least in the sense that they’re susceptible to SARS-CoV-2 infection, according to serum samples from the Department of Agriculture’s Animal and Plant Health Inspection Service.
Vaccinated people should be tested for COVID-19 and mask up after coming into contact with an infected person, according to updated CDC guidelines released this week. The change quietly accompanied the agency’s new masking recommendations for areas of substantial and high transmission and K-12 schools, as data continue to accrue about the more transmissible Delta variant and the risk for vaccinated people contracting and spreading the virus.
The U.S. government will pay for the testing Biden ordered for unvaccinated federal workers.
Dr. Gottlieb estimates up to 1 million Americans being infected with Covid daily
Today’s Posts On Econintersect Showing Impact Of The Pandemic and Recovery With Hyperlinks
23 July 2021 ECRI’s WLI Growth Rate Decline Continues
Final July 2021 Michigan Consumer Sentiment Improves Slightly From Preliminary
July 2021 Chicago Purchasing Managers Barometer Significantly Improves
June 2021 Real Income And Expenditures – Inflation Continues To Impact
Pfizer Gets A Booster Shot From Its COVID-19 Vaccine
GDP Growth Number Greatly Enhanced By ‘Optimistic’ Deflator
Warning to Readers
The amount of politically biased articles on the internet continues. And studies and opinions of the experts continue to contradict other studies and expert opinions. Honestly, it is difficult to believe anything anymore.

I assemble this update daily – sifting through the posts on the internet. I try to avoid politically slanted posts. This daily blog is not an echo chamber for any party line – and will publish controversial topics unless there are clear reasons why the topic is false. And I usually publish conflicting topics. It is my job to provide information so that you have the facts necessary – and then it is up to readers to draw conclusions. It is not my job to sell any point of view.
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- Older population countries will have a significantly higher death rate as there is relatively few hospitalizations and deaths in younger age groups..
What we do or do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work. Unfortunately, early in the pandemic, many health experts — in the U.S. and around the world — decided that the public could not be trusted to hear the truth about masks. Instead, the experts spread a misleading message, discouraging the use of masks.
- Current thinking is that we develop at least 12 months of immunity from further COVID infection.
- The Moderna and Pfizer vaccines have an effectiveness rate of about 95 percent after two doses. That is on par with the vaccines for chickenpox and measles. The 95 percent number understates the effectiveness as it counts anyone who came down with a mild case of Covid-19 as a failure.
- To what degree do people who never develop symptoms contribute to transmission? Research early in the pandemic suggested that the rate of asymptomatic infections could be as high as 81%. But a meta-analysis, which included 13 studies involving 21,708 people, calculated the rate of asymptomatic presentation to be 17%.
- The accuracy of rapid testing is questioned – and the more accurate test results are not being given in a timely manner.
- Can children widely spread coronavirus? [current thinking remains that they are a minor source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- Air conditioning contributes to the pandemic spread.
- It appears that there is increased risk of infection and mortality for those living in larger occupancy households.
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>





