Written by Steven Hansen
The U.S. new cases 7-day rolling average are 16.7 % LOWER than the 7-day rolling average one week ago and U.S. deaths due to coronavirus are now 3.9 % LOWER than the rolling average one week ago. Today’s posts include:
- U.S. Coronavirus New Cases are 22,391
- U.S. Coronavirus deaths are at 246
- U.S. Coronavirus immunizations have been administered to 77.0 doses per 100 people.
- The 7-day rolling average rate of growth of the pandemic shows new cases improved and deaths improved
- Chinese Military Discussed Weaponizing COVID In 2015 ‘To Cause Enemy’s Medical System To Collapse’
- Origins of COVID-19: Who Opened Pandora’s Box at Wuhan – People or Nature?
- How the US Locked Up Vaccine Materials Other Nations Urgently Need
- BioNTech CEO: Patent waivers are not needed
- CDC Limits Review of Vaccinated but Infected; Draws Concern
- Are the Immunosuppressed Responding to Two Doses?
- New vaccine blocks COVID-19 and variants, plus other coronaviruses
- The world may need to learn to live with the virus
- Plus loads of headlines today not mentioned above

include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus1.htm’); ?>
Hospitalizations Are The Only Accurate Gauge
Hospitalizations historically appear to be little affected by weekends or holidays. The hospitalization growth rate trend continues to improve.

source: https://gis.cdc.gov/grasp/covidnet/COVID19_3.html
Historically, hospitalization growth follows new case growth by one to two weeks.
As an analyst, I use the rate of growth to determine the trend. But, the size of the pandemic is growing in terms of real numbers – and if the rate of growth does not become negative – the pandemic will overwhelm all resources.
The graph below shows the rate of growth relative to the growth a week earlier updated through today [note that negative numbers mean the rolling averages are LOWER than the rolling averages one week ago]. As one can see, the rate of growth for new cases peaked in early December 2020 for Thanksgiving, and early January 2021 for end-of-year holidays – and it now shows that the coronavirus effect is improving.

In the scheme of things, new cases decline first, followed by hospitalizations, and then deaths. The potential fourth wave did not materialize likely due to immunizations.
Coronavirus News You May Have Missed
Chinese Military Discussed Weaponizing COVID In 2015 ‘To Cause Enemy’s Medical System To Collapse’ – ZeroHedge
In 2015, Chinese military scientists discussed how to weaponze SARS coronaviruses, five years before the COVID-19 pandemic emerged in Wuhan, China – where CCP scientists were collaborating with a US-funded NGO on so-called ‘gain of function’ research to make bat coronaviruses infect humans more easily.
In a 263-page document, written by People’s Liberation Army scientists and senior Chinese public health officials and obtained by the US State Department during its investigation into the origins of COVID-19, PLA scientists note how a sudden surge of patients requiring hospitalization during a bioweapon attack “could cause the enemy’s medical system to collapse,” according to The Weekend Australian (a subsidiary of News Corp).
It suggests that SARS coronaviruses could herald a “new era of genetic weapons,” and noted that they can be “artificially manipulated into an emerging human disease virus, then weaponized and unleashed in a way never seen before.”
The chairmen of the British and Australian foreign affairs and intelligence committees, Tom Tugendhat and James Paterson, say the document raises major concerns about China’s lack of transparency over the origins of COVID-19.
The Chinese-language paper, titled The Unnatural Origin of SARS and New Species of Man-Made Viruses as Genetic Bioweapons, outlines China’s progress in the research field of biowarfare.
“Following developments in other scientific fields, there have been major advances in the delivery of biological agents,” it states.
“For example, the new-found ability to freeze-dry micro-organisms has made it possible to store biological agents and aerosolise them during attacks.”
Ten of the authors are scientists and weapons experts affiliated with the Air Force Medical University in Xi’an, ranked “very high-risk” for its level of defence research, including its work on medical and psychological sciences, according to the Australian Strategic Policy Institute’s Defence Universities Tracker.
The Air Force Medical University, also known as the Fourth Medical University, was placed under the command of the PLA under President Xi Jinping’s military reforms in 2017. The editor-in-chief of the paper, Xu Dezhong, reported to the top leadership of the Chinese Military Commission and Ministry of Health during the SARS epidemic of 2003, briefing them 24 times and preparing three reports, according to his online biography. -The Australian
“We were able to verify its authenticity as a document authored by the particular PLA researchers and scientists,” according to Robert Potter, a digital forensics specialist who has worked for the US, Australian and Canadian governments – and has previously analyzed leaked Chinese government documents, according to the report. “We were able to locate its genesis on the Chinese internet.”
Former US Secretary of State Mike Pompeo and his chief China adviser, Miles Yu, referenced the document in a February op-ed in the Wall Street Journal, writing that “A 2015 PLA study treated the 2003 SARS coronavirus outbreak as a ‘contemporary genetic weapon’ launched by foreign forces.”
Are the Immunosuppressed Responding to Two Doses? – MedPage
Back in March, we published in JAMA and reported here in MedPage Today that only 17% of immunosuppressed transplant patients — in stark contrast to 100% of immunocompetent people — mounted detectable antibodies to SARS-CoV-2 after the first dose of mRNA vaccine. Our report was among the top five most read articles in JAMA, and generated substantial — and understandable — concern among communities of immunosuppressed people. As a transplant surgeon, I was frustrated and frightened for my patients, and my Johns Hopkins colleagues and I eagerly awaited the results looking at antibody response after full two-dose vaccination.
The moment many transplant patients and physicians have been waiting for has finally arrived, but unfortunately the news is not great. We have now published in JAMA second-dose data from our national study of vaccine immune responses in immunosuppressed solid organ transplant recipients. Among 658 COVID-19-naïve participants who received the full two-dose series of mRNA vaccines, 46% (compared to 83% after just one dose) still had no detectable antibodies, and even among those with detectable antibodies, the levels were still somewhat low. The situation is worse among those taking anti-metabolites: for this group, 57% had no antibodies after full vaccination, compared to 32% with no antibodies among those not taking anti-metabolites.
Unfortunately, this blunted antibody response seems to correlate with diminished protective immunity. We are seeing in our own patients, and hearing from around the country, many cases of transplant patients receiving a full vaccine series, thinking they are immune, believing that the CDC guidelines for vaccinated people apply to them, relaxing the masking and distancing behaviors that have protected them for over a year, and sadly finding themselves hospitalized with a new COVID-19 infection. Some have even died. This is highly problematic. We need more effort and action to spread the word that vaccination does not necessarily mean immunity in this vulnerable population.
So, what should our transplant patients do in light of these findings? First and foremost, they should continue to practice all the protective behaviors they have thus far practiced. While the rest of the world is celebrating the new freedoms that come with vaccination, unfortunately the time is not yet right for transplant patients to do so. Eventually we will understand the immune response to vaccines in our patients enough to relax these restrictions, but right now we only know the impact on antibody response (with very little understanding of memory B cell and T cell response, which are both important), and what we know is not encouraging. Transplant patients should also make sure that everyone around them gets vaccinated, so at least their environments are safer. And, of course, this is yet another reason that everyone should want to get vaccinated — to protect the vulnerable who cannot achieve immunity for themselves, and ultimately help reach herd immunity.
Origins of COVID-19: Who Opened Pandora’s Box at Wuhan – People or Nature? – The Wire
Natural emergence was the media’s preferred theory until around February 2021 and the visit by a World Health Organization commission to China. The commission’s composition and access were heavily controlled by the Chinese authorities. Its members, who included the ubiquitous Dr. Daszak, kept asserting before, during and after their visit that lab escape was extremely unlikely. But this was not quite the propaganda victory the Chinese authorities may have been hoping for. What became clear was that the Chinese had no evidence to offer the commission in support of the natural emergence theory.
This was surprising because both the SARS1 and MERS viruses had left copious traces in the environment. The intermediary host species of SARS1 was identified within four months of the epidemic’s outbreak, and the host of MERS within nine months. Yet some 15 months after the SARS2 pandemic began, and a presumably intensive search, Chinese researchers had failed to find either the original bat population, or the intermediate species to which SARS2 might have jumped, or any serological evidence that any Chinese population, including that of Wuhan, had ever been exposed to the virus prior to December 2019. Natural emergence remained a conjecture which, however plausible to begin with, had gained not a shred of supporting evidence in over a year.
And as long as that remains the case, it’s logical to pay serious attention to the alternative conjecture, that SARS2 escaped from a lab.
[editor’s note: this is just the tip of the iceberg from this well written post. Recommend a full read
CDC Limits Review of Vaccinated but Infected; Draws Concern – Bloomberg
Federal health officials this month decided to limit how they monitor vaccinated people who have been infected with Covid-19, drawing concern from some scientists who say that may mean missing needed data showing why and how it happens.
At the end of April, more than 9,000 Americans were reported to be infected after being vaccinated, according to the U.S. Centers for Disease Control and Prevention. While that’s a tiny percentage of the 95 million people fully inoculated at the time, researchers still want to find out what specific mechanisms may be spurring the infections.
Rare breakthrough cases are expected since no vaccines are 100% effective. But tracking and sequencing the cases helps in figuring out who may be more at risk, whether new variants evade the vaccines and when protection from the shots begins to wane. At the same time, those infected — some of whom are suffering widespread medical issues, even if they’re not hospitalized — say they feel lost as a result of the lack of information.
“We shouldn’t be narrowing the focus, we should be broadening and develop a systematic plan,” said Eric Topol, director of the Scripps Research Translational Institute in La Jolla.
At the start of May, the CDC shifted from monitoring all reported breakthroughs to only those that result in hospitalization or death, Tom Clark, head of the vaccine evaluation unit for the CDC’s vaccine task force, said in an interview. The goal of the new strategy, according to the agency: maximize the quality of data collected on cases.
TOTAL NUMBER OF BREAKTHROUGH INFECTIONS REPORTED TO CDC 9,245 Females 5,827 (63%) People aged 60 and older 4,245 (45%) Asymptomatic infections 2,525 (27%) Hospitalizations 835 (9%) Deaths 132 (1%) The CDC says its numbers are probably an undercount, since their surveillance system is passive and relies on voluntary reporting from state health departments that may not be complete.
The agency shifted its strategy because there’s few worrying patterns in the data collected so far, suggesting the focus should be on the most severe cases, Clark said. He added that the agency has planned other vaccine studies, including one with a network of health centers, to compare disease severity and frequency of variant infections between vaccinated and unvaccinated people.
New vaccine blocks COVID-19 and variants, plus other coronaviruses – EurekAlert
A potential new vaccine developed by members of the Duke Human Vaccine Institute has proven effective in protecting monkeys and mice from a variety of coronavirus infections — including SARS-CoV-2 as well as the original SARS-CoV-1 and related bat coronaviruses that could potentially cause the next pandemic.
The new vaccine, called a pan-coronavirus vaccine, triggers neutralizing antibodies via a nanoparticle. The nanoparticle is composed of the coronavirus part that allows it to bind to the body’s cell receptors and is formulated with a chemical booster called an adjuvant. Success in primates is highly relevant to humans.
The findings appear Monday, May 10, in the journal Nature.
“We began this work last spring with the understanding that, like all viruses, mutations would occur in the SARS-CoV-2 virus, which causes COVID-19,” said senior author Barton F. Haynes, M.D., director of the Duke Human Vaccine Institute (DHVI). “The mRNA vaccines were already under development, so we were looking for ways to sustain their efficacy once those variants appeared.
“This approach not only provided protection against SARS-CoV-2, but the antibodies induced by the vaccine also neutralized variants of concern that originated in the United Kingdom, South Africa and Brazil,” Haynes said. “And the induced antibodies reacted with quite a large panel of coronaviruses.”
How the US Locked Up Vaccine Materials Other Nations Urgently Need – Medscape
To fight the pandemic at home, the United States gave its own vaccine manufacturers priority access to American-made materials needed to make the shots.
As a result, the U.S. government laid claim not only to vast quantities of finished COVID-19 vaccines but also to vaccine components and equipment all along the supply chain, according to a Reuters review of more than a dozen contracts involving some major suppliers.
That has left some countries desperately in need of those supplies to scramble for substitutes, exacerbating international disparities in vaccine access, according to interviews with suppliers, foreign manufacturers and vaccine market experts.
On Wednesday, President Joe Biden threw his support behind waiving patents for COVID-19 vaccines, thrilling those who have been pressuring his administration to help speed production of doses worldwide. If adopted by the World Trade Organization, the move would let other countries make their own copies of the much-coveted shots.
But the waiver would not address a less conspicuous but equally pressing problem: the growing worldwide shortage of vaccine ingredients and manufacturing equipment. The United States has a tight grip on a significant amount of those materials, such as filters, tubing and specialized disposable bags essential to making vaccines.
Countries ravaged by the virus – including India, where a catastrophic explosion of cases has filled hospitals and morgues – cannot make vaccines without such supplies, even with access to manufacturers’ cookbooks.
The problem stems from the U.S. reliance on a law dating to the Korean War in the 1950s, called the Defense Production Act (DPA), which gives federal agencies the power to prioritize procurement orders related to national defense. For decades, the law was used to supply the military as well as respond to everything from natural disasters to roadblocks in the decennial U.S. census.
The administration of former President Donald Trump invoked the act to put the U.S. government first in line to buy American-made vaccines as well as other products needed to fight the COVID-19 pandemic. In turn, vaccine makers have priority access to any supplies needed to fill U.S. orders.
BioNTech CEO: Patent waivers are not needed – The Hill
The CEO of German coronavirus vaccine maker BioNTech said Monday he does not see a need to waive intellectual property protections, because there will be enough supply in the coming year for the rest of the world.
“We believe, together with the other vaccine developers, in the next 9 to 12 months, that there will be more than enough vaccine produced, and there is absolutely no need for waiving patents,” Ugur Sahin said during a call with investors and analysts.
BioNTech recorded a net profit of 1.13 billion euros, or $1.37 billion, for the first three months of 2021, compared to a net loss of 53.4 million euros for the first quarter last year.
The Biden administration made waves last week when it announced support for a waiver of intellectual property and patent protections for vaccines at the World Trade Organization. Supporters of the move argue it would enable lower-income countries to gain access to vaccine recipes and start making more doses themselves.
The pharmaceutical industry, however, claims the waiver will undermine incentives for American innovation and will not actually solve the complex problem of getting more doses to lower-income countries.
Sahin echoed those arguments on Monday, saying that waiving patents would not increase short- and medium-term supply of mRNA vaccines. Setting up manufacturing for the vaccines is complex, he said, and will take at least a year.
The world may need to learn to live with the virus. – New York Times
Experts now say it is changing too quickly, new more contagious variants are spreading too easily and vaccinations are happening too slowly for herd immunity to be within reach anytime soon.
That means if the virus continues to run rampant through much of the world, it is well on its way to becoming endemic, an ever-present threat.
Virus variants are tearing through places where people gather in large numbers with few or no pandemic protocols, like wearing masks and distancing, according to Dr. David Heymann, a professor of infectious disease epidemiology at the London School of Hygiene and Tropical Medicine.
While the outbreak in India is capturing the most attention, Dr. Heymann said the pervasive reach of the virus means that the likelihood is growing that it will persist in most parts of the world.
As more people contract the virus, developing some level of immunity, and the pace of vaccinations accelerates, future outbreaks won’t be on the scale of those devastating India and Brazil, Dr. Heymann said. Smaller outbreaks that are less deadly but a constant threat should be expected, Dr. Heymann said.
“This is the natural progression of many infections we have in humans, whether it is tuberculosis or H.I.V.,” said Dr. Heymann, a former member of the Epidemiology Intelligence Service at the Centers for Disease Control and Prevention and a former senior official at the World Health Organization. “They have become endemic and we have learned to live with them and we learn how to do risk assessments and how to protect those we want to protect.”
The following are foreign headlines with hyperlinks to the posts
After a slow start to its vaccination campaign, the European Union is administering nearly three million doses a day.
Hit by COVID, Senegal’s women find renewed hope in fishing
British officials said individuals younger than age 40 should be offered an alternative to AstraZeneca’s vaccine, given the reports of rare blood clots in younger adults.
The safety committee of the European Medicines Agency said it is monitoring cases of Guillain-Barre syndrome among AstraZeneca vaccine recipients and is aware of cases of inflammation of heart muscle and membrane following administration of the Pfizer vaccine, but there is no indication of a causal relationship between the two.
The World Health Organization bestowed emergency approval on Chinese company Sinopharm’s COVID-19 vaccine, the first vaccine by a non-Western company to be approved by the WHO.
An outgoing vaccine task force official in Britain said the coronavirus will no longer be circulating in the U.K. by August.
A team led by Professor Burkhard Becher at the Institute of Experimental Immunology at the University of Zurich, working with researchers from Tübingen, Toulouse and Nantes, has now discovered First biomarker to predict severity of COVID – the number of natural killer T cells in the blood. These cells are a type of white blood cell and part of the early immune response. “The number of natural killer T cells in the blood can be used to predict severe cases of COVID-19 with a high degree of certainty – even on a patient’s first day in hospital,” says Burkhard Becher.
Cardiac complications found to be rare in college athletes who contracted COVID-19
Key EU Countries Rebuff Biden on Sharing COVID Vaccine Patents
Amid COVID Outbreaks on Mount Everest, China Keeping Nepal Climbers Away
Nepal official calls the pandemic an “overwhelming burden” days after saying it was “under control”
Indians Converting Cricket Stadium, University into COVID Hospitals
Saudi Arabia says pilgrimage to Mecca will be allowed, but the rules remain unclear.
Malaysia imposes nationwide lockdown during 3rd wave of coronavirus
Unequal access to Covid immunization amounts to “vaccine apartheid,” says South African President
Germany to offer Johnson & Johnson vaccine to all adults
Hundreds party as coronavirus curfew ends in most of Spain
Sri Lanka reports new record-high number of Covid-19 cases in a day
The following additional national and state headlines with hyperlinks to the posts
Several states — including Wisconsin, Iowa and the Carolinas — have asked the federal government to send fewer doses as U.S. demand continues to fall.
Most schools have reopened, at least partly. But students continue to opt out of in-person classes — often for reasons beyond the virus.
NIAID Director Anthony Fauci, MD, predicted that indoor masking guidance may soon be relaxed as more people get vaccinated.
Latest CDC data indicate that 58% of U.S. adults have received at least their first dose of COVID-19 vaccine, with 44% fully vaccinated.
U.S. cases down 30% over the past two weeks, averaging 2 million shots per day
AstraZeneca may forgo asking for emergency use authorization for its COVID-19 vaccine and instead apply for full approval.
Researchers show SARS-CoV-2 genes can be integrated into the human genome
Combo COVID-flu vaccine protects against current and emerging variants in animal model
Biden: Workers can’t turn down job and get benefits
California scores staggering $75B budget surplus
Woman Accidentally Vaccinated With Six Pfizer Doses
Treasury will give states a lot of power to decide how to spend $350 billion in Covid relief funds
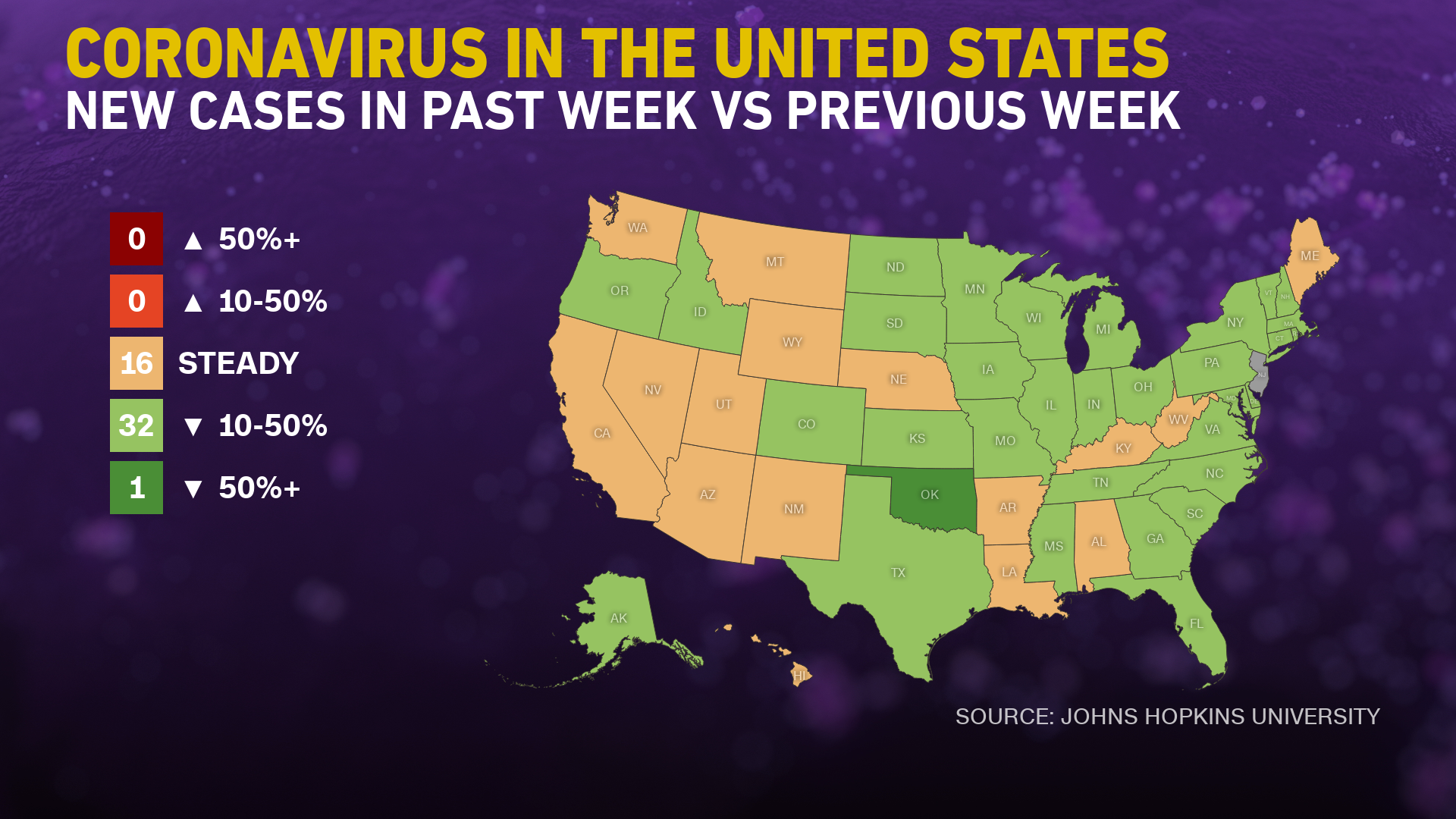
No US state is reporting an increase in coronavirus cases
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
April 2021 Conference Board Employment Index: Shows No Signs Of Slowing Job Growth
Credit Card Deleveraging During The COVID-19 Pandemic
US Dollar Share Of Global Foreign Exchange Reserves Drops To 25-Year Low
The Last Resort In A Changing Landscape
Telemedicine Is A Tool Not A Replacement For Your Doctors Touch
Warning to Readers
The amount of politically biased articles on the internet continues. And studies and opinions of the experts continue to contradict other studies and expert opinions. Honestly, it is difficult to believe anything anymore.

I assemble this coronavirus update daily – sifting through the posts on the internet. I try to avoid politically slanted posts (mostly from CNN, New York Times, and the Washington Post) and can usually find unslanted posts on that subject from other sources on the internet. I wait to publish posts on subjects that I cannot validate across several sources. But after all this extra work, I do not know if I have conveyed the REAL facts. It is my job to provide information so that you have the facts necessary – and then it is up to readers to draw conclusions.
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19 when recovering from COVID-19. Herd immunity does not look like an option without immunization although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a significantly higher death rate as there is relatively few hospitalizations and deaths in younger age groups..
- There are at least 8 strains of the coronavirus. California and New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
What we do or do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work. Unfortunately, early in the pandemic, many health experts — in the U.S. and around the world — decided that the public could not be trusted to hear the truth about masks. Instead, the experts spread a misleading message, discouraging the use of masks.
- Current thinking is that we develop at least 12 months of immunity from further COVID infection.
- The Moderna and Pfizer vaccines have an effectiveness rate of about 95 percent after two doses. That is on par with the vaccines for chickenpox and measles. The 95 percent number understates the effectiveness as it counts anyone who came down with a mild case of Covid-19 as a failure.
- To what degree do people who never develop symptoms contribute to transmission? Research early in the pandemic suggested that the rate of asymptomatic infections could be as high as 81%. But a meta-analysis, which included 13 studies involving 21,708 people, calculated the rate of asymptomatic presentation to be 17%.
- The accuracy of rapid testing is questioned – and the more accurate test results are not being given in a timely manner.
- Can children widely spread coronavirus? [current thinking is that they are a minor source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- Air conditioning contributes to the pandemic spread.
- It appears that there is increased risk of infection and mortality for those living in larger occupancy households.
- Male patients have almost three times the odds of requiring intensive treatment unit (ITU) admission compared to females.
- Outdoor activities seem to be a lower risk than indoor activities.
Treatments with solid scientific support:
- Dexamethasone
- Proning, or turning someone on their stomach
- Remdesivir
- Baricitinib
Treatments with potential but limited evidence:
- ECMO, or extracorporeal membrane oxygenation
- fluvoxamine
- Cyclosporine
- Famotidine
- Intravenous immunoglobulin
- Ivermectin
- Interferons
Drugs shown to be ineffective:
- The combination of lopinavir-ritonavir
- Hydroxychloroquine
- Insulin
- High dose zinc and vitamin C
- Convalescent plasma
- Monoclonal antibodies
- Tocilizumab
- Anti-coagulants
- A current scientific understanding of the way the coronavirus works can be found [here].
There is now a vaccine available – the questions remain:
- will there be any permanent side effects that will appear months from now,
- how long immunity will last [we can currently say we do not know if it will last more than 4 months],
- there is no solid evidence yet the vaccine will block transmission
Heavy breakouts of coronavirus have hit farmworkers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>





