Written by Steven Hansen
The U.S. new cases 7-day rolling average are 12.4 % LOWER than the 7-day rolling average one week ago and U.S. deaths due to coronavirus are now 4.3 % LOWER than the rolling average one week ago. Today’s posts include:
- U.S. Coronavirus New Cases are 65,471
- U.S. Coronavirus deaths are at 901
- U.S. Coronavirus immunizations have been administered to 64.6 % of the population
- The 7-day rolling average rate of growth of the pandemic shows new cases improved and deaths worsened
- CDC advisers recommend resuming use of Johnson & Johnson coronavirus vaccine
- New Study Shows “Long Haul” COVID-19 Can Kill Patients Months After Infection
- High dose of vitamin D fails to improve the condition of moderate to severe COVID-19 patients
- Can We Get to ‘COVID Zero’? Experts Predict Next 8 Months
- Only one vaccine is OK for older teens. It’s also the hardest to manage in rural America
- British regulator says AstraZeneca COVID shot clots rise to 168
- Drop in vaccine demand has some places turning down doses
- Drug Repurposing for COVID-19: What Went Wrong?
- Texas Ended Lockdowns & Mask Mandates; Now Locked-Down States Are Where COVID Is Growing Most
- Many other interesting headlines today!

include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus1.htm’); ?>
Hospitalizations Are The Only Accurate Gauge
Hospitalizations historically appear to be little affected by weekends or holidays. The hospitalization growth rate trend is improving.

source: https://gis.cdc.gov/grasp/covidnet/COVID19_3.html
Historically, hospitalization growth follows new case growth by one to two weeks.
As an analyst, I use the rate of growth to determine the trend. But, the size of the pandemic is growing in terms of real numbers – and if the rate of growth does not become negative – the pandemic will overwhelm all resources.
The graph below shows the rate of growth relative to the growth a week earlier updated through today [note that negative numbers mean the rolling averages are LOWER than the rolling averages one week ago]. As one can see, the rate of growth for new cases peaked in early December 2020 for Thanksgiving, and early January 2021 for end-of-year holidays – and it now shows that the coronavirus effect is lower.

In the scheme of things, new cases decline first, followed by hospitalizations, and then deaths.
The New Variants Are The Primary Cause Of This Fourth Wave
Even with vaccinations picking up, the fourth wave is now underway.
- the more people that are vaccinated reduces the pool of people that can be infected. Today we have removed over 64 % of the population from being infected which theoretically should reduce the infection rate by 64 % [it is unproven whether the vaccines prevent a vaccinated person from being a carrier of the virus even though showing no signs]. If the vaccines are shown to stop transmission, then in theory it would reduce the infection rate by double the percent vaccinated [in this case you prevent your own infection and do not pass it along to another].
- it is also unknown what the effective rate of the current vaccines is against mutations that seem to appear almost daily. As an example, if the effective rate drops to 60%, it means the 64 % reduction in the infection rate discussed above is almost cut in half. The South African and Brazilian variant is reported somewhat immune to the current vaccines.
- In theory, the pandemic should be over immediately if everyone could be vaccinated today. The problem is that every day brings a new mutation (which would not appear if the pandemic was stopped). The longer the immunization process takes – the more ineffective the vaccine will become.
- It is not clear whether the vaccine prevents those vaccinated from spreading the virus. It seems to be well documented that it normally stops the virus from taking hold and when it does not – the infection is mild.
The real question is whether the vaccines will be mitigating this surge – and to what extent.
Coronavirus News You May Have Missed
Vaccine advisers to the US Centers for Disease Control and Prevention are considering four choices for changing the agency’s recommendation on Johnson & Johnson’s coronavirus vaccine, including label changes or a complete end to its use.
The CDC’s Advisory Committee on Immunization Practices is holding an emergency meeting and is expected to vote later Friday on recommendations.
At issue: The vaccine has been linked to 15 cases of a rare blood clotting condition called thrombosis with thrombocytopenia syndrome, or TTS, all among women. Three have died.
The committee’s four possible choices are:
- Recommend against use for all persons
- Reaffirm recommendation for all age and sex – US Food and Drug Administration to include warning statement with emergency use authorization
- Recommend vaccination only for adults aged 50 or older
- Reaffirm recommendations for use; women aged under 50 should be aware of the increased risk of TTS, and may choose another Covid-19 vaccine (ie mRNA vaccines)
Earlier, Johnson & Johnson officials said they had agreed with the FDA on new wording to add to the label saying the risk of blood clots is plausible and warning of the risks.
CDC advisers recommend resuming use of Johnson & Johnson coronavirus vaccine – CNN
Vaccine advisers to the US Centers for Disease Control and Prevention voted Friday to recommend resuming use of the Johnson & Johnson coronavirus vaccine.
Members of the CDC’s Advisory Committee for Immunization Practices agreed the benefits of the vaccine outweigh the risks from rare blood clots linked with the vaccine.
The language of the vote said: “The Janssen Covid-19 vaccine is recommended for persons 18 years of age and older in the U.S. population under the FDA’s emergency use authorization.”
“The vote is 10 in favor, four opposed and one abstention. The motion carries,” Dr. Jose Romero, Arkansas secretary of health and chair of ACIP, said.
More context: The US Food and Drug Administration will update the label for the vaccine, indicating that women under the age of 50 should be aware of the risk of blood clots from the vaccine.
Earlier, Johnson & Johnson officials said they had agreed to updated language for the label.
CDC Director Dr. Rochelle Walensky will sign off and then the US Food and Drug Administration will prepare an amended emergency use authorization for the vaccine, Dr. Amanda Cohn, ACIP’s executive secretary, said at the meeting earlier.
“We are awaiting and anticipate that the FDA will be putting out a new, a newly approved EUA language,” Cohn said. “And additionally, we will be taking the input from today, along with this language that FDA will publish and both FDA and CDC will have communication materials and education materials including infographics, patient fact sheets.”
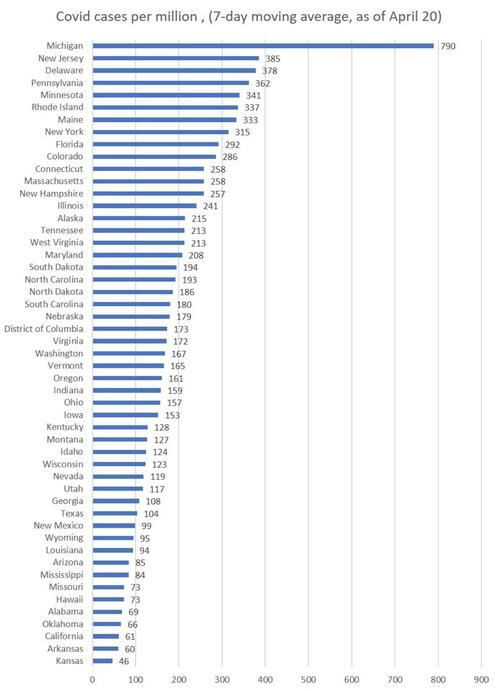
Texas Ended Lockdowns & Mask Mandates; Now Locked-Down States Are Where COVID Is Growing Most – ZeroHedge
Early last month, Texas governor Greg Abbott announced he would end the state’s mask mandate and allow most businesses to function at 100 percent capacity.
The response from the corporate media and the Left was predictable. California governor Gavin Newsom declared the move “absolutely reckless.” Beto O’Rourke called the GOP a “cult of death.” Joe Biden called the move “Neanderthal thinking.” Keith Olbermann insisted, “Texas has decided to join the side of the virus” and suggested Texans shouldn’t be allowed to take the covid vaccine. Vanity Fair ran an article with the title “Republican Governors Celebrate COVID Anniversary with Bold Plan to Kill Another 500,000 Americans.”
Georgia and Florida, of course, are both notable for ending lockdowns and restriction much earlier than many other states. And in those cases as well, the state governments were criticized for their policies, which were said to be reckless and sure to lead to unprecedented death. Georgia’s policy was denounced as an experiment in “human sacrifice.”
Yet in recent weeks, these predictions about Texas’s fate have proven to be spectacularly wrong. Moreover, many of the states with the worst growth in covid cases-and the worst track records in overall death counts-have been states that have had some of the harshest lockdowns. The failure of the lockdown narrative in this case has been so overwhelming that last week, when asked about the Texas situation, Anthony Fauci could only suggest a few unconvincing lines about how maybe Texans are voluntarily wearing masks and locking down more strenuously than people in other states. In Fauci’s weak-sauce explanation we see a narrative that simply fails to explain the actual facts of the matter.
Patients With Long Covid Face Lingering Worrisome Health Risks, Study Finds – New York Times
Patients who were not sick enough to be hospitalized still had a significantly greater risk of dying within six months than people who were not infected.
The health effects of Covid-19 not only can stretch for months but appear to increase the risk of death and chronic medical conditions, even in people who were never sick enough to be hospitalized, a large new study finds.
In the study, published Thursday in the journal Nature, researchers looked at medical records of more than 73,000 people across the United States whose coronavirus infections did not require hospitalization. Between one and six months after becoming infected, those patients had a significantly greater risk of death – 60 percent higher – than people who had not been infected with the virus.
The research, based on records of patients in the Department of Veterans Affairs health system, also found that nonhospitalized Covid survivors had a 20 percent greater chance of needing outpatient medical care over those six months than people who had not contracted the coronavirus.
The Covid survivors experienced a vast array of long-term medical problems that they had never had before – not just lung issues from the respiratory effects of the virus, but symptoms that could affect virtually any organ system or part of the body, from neurological to cardiovascular to gastrointestinal. They were also at greater risk of mental health problems, including anxiety and sleep disorders.
… What’s more, some of the patients’ post-Covid medical issues – like diabetes, kidney disease and some heart problems – could become chronic conditions that would require treatment for the rest of their lives.
[editor’s note: also read New Study Shows “Long Haul” COVID-19 Can Kill Patients Months After Infection]
Drug Repurposing for COVID-19: What Went Wrong? – MedPage
So far in the pandemic, support for research on drug repurposing — particularly for inexpensive generics — has not played a huge role in finding new treatments for COVID-19, but that appears to be changing.
Critics charge that drug repurposing is like looking for a needle in a haystack. It does not always work, and can raise false hopes and waste resources. In a March 7 interview with 60 Minutes, for instance, NIH director Francis Collins, MD, PhD, said drug repurposing “is only going to work if you’re kind of lucky, because you’re basically picking things that were developed for a different disease.”
Proponents say that the strategy can be faster and cheaper than de novo drug development. About 90% of de novo drugs fail at some point during development, and it can take 10 to 12 years and cost $2 to $3 billion for the winners to come to market. In contrast, the average repurposed drug can rely on past safety data to speed its development, and costs about $300 million to bring to market, according to a 2020 report by Roots Analysis.
Those proponents are now finding their voices heard. As part of NIH’s Accelerating COVID-19 Therapeutic Interventions and Vaccines (ACTIV) trial program, ACTIV-6 was launched to examine up to seven repurposed drugs for their efficacy in treating mild-to-moderate COVID-19 outpatients.
Feds Overlooked Repurposing, at What Cost?
Early in the pandemic, the U.S. failed to evaluate repurposed drugs for COVID-19 and “pursued an almost singular focus on vaccines that was very unusual and clearly driven by leadership,” charges Rena Conti, PhD, associate research director of the Institute for Health System Innovation and Policy at the Questrom School of Business at Boston University.
… While the U.S. was preoccupied with hydroxychloroquine, the U.K. organized the RECOVERY study, a six-arm trial that validated the mortality benefit of dexamethasone in the treatment of hospitalized patients with COVID-19, and early on showed lack of benefit for hydroxychloroquine in hospitalized patients.
To be fair, the NIH did support the ORCHID trial, which confirmed no beneficial effect for hydroxychloroquine in hospitalized patients with COVID-19, but at the cost of wasting scarce time and resources, Conti said. RECOVERY has been “incredibly cost effective and highly productive,” ringing up at about $20 million, a “drop in the bucket” compared to what the U.S. spent on Zika, Ebola, or H1N1, according to Conti.
The NIH also supported early-stage drug repurposing research via the National Center for Advancing Translational Sciences (NCATS). NCATS did high-throughput screening of thousands of approved compounds, and made their data sets publicly available.
Drop in vaccine demand has some places turning down doses – AP
Louisiana has stopped asking the federal government for its full allotment of COVID-19 vaccine. About three-quarters of Kansas counties have turned down new shipments of the vaccine at least once over the past month. And in Mississippi, officials asked the federal government to ship vials in smaller packages so they don’t go to waste.
As the supply of coronavirus vaccine doses in the U.S. outpaces demand, some places around the country are finding there’s such little interest in the shots, they need to turn down shipments.
“It is kind of stalling. Some people just don’t want it,” said Stacey Hileman, a nurse with the health department in rural Kansas’ Decatur County, where less than a third of the county’s 2,900 residents have received at least one vaccine dose.
The dwindling demand for vaccines illustrates the challenge that the U.S. faces in trying to conquer the pandemic while at the same time dealing with the optics of tens of thousands of doses sitting on shelves when countries like India and Brazil are in the midst of full-blown medical emergencies.
More than half of American adults have received at least one vaccine dose, and President Joe Biden this week celebrated eclipsing 200 million doses administered in his first 100 days in office. He also acknowledged entering a new phase to bolster outreach and overcome hesitancy.
Across the country, pharmacists and public health officials seeing the demand wane and supplies build up. About half of Iowa’s counties have stopped asking for new doses from the state, and Louisiana didn’t seek shipment of some vaccine doses over the past week.
In Mississippi, small-town pharmacist Robin Jackson has been practically begging anyone in the community to show up and get shots after she received her first shipment of vaccine earlier this month and demand was weak, despite placing yard signs outside her storefront celebrating the shipment’s arrival. She was wasting more vaccine than she was giving out and started coaxing family members into the pharmacy for shots.
“Nobody was coming,” she said. “And I mean no one.”
Should We Be Vaccinating Dogs And Cats For COVID? [my headline not the one used by the CDC] – CDC
Because SARS-CoV-2 can infect cats and dogs, the virus might spread in this population and animals might act as a reservoir with the possibility of animal-to-human transmission. Although so far the pandemic has been driven by human-to-human transmission, it is useful to know whether domestic animals can play a role in maintenance and spread of SARS-CoV-2 infections, as underscored by the recent reports that workers from mink farms had acquired SARS-CoV-2 from minks (24,25). For these studies, verified serologic assays that detect virus-specific antibody responses in cats and dogs are needed. In our study, we modified assays used in human epidemiologic studies and validated ELISAs to detect SARS-CoV-2 S1 and RBD antibodies and VN by using pseudotyped SARS2-VSV for screening cat and dog samples. We defined seropositivity on the basis of results for positive samples from the SARS-CoV-2-exposed cohort.
British regulator says AstraZeneca COVID shot clots rise to 168 – Reuters
Britain’s medicines regulator on Thursday said there had been 168 major blood clots following a dose of AstraZeneca’s (AZN.L) COVID-19 vaccine, a rate of 7.9 clots per million doses, a jump in incidence from the previous week’s figure.
This was up from the 100 cases reported last week, when the overall case incidence was 4.9 per million doses.
There has been scrutiny of the AstraZeneca vaccine on the issue of the very rare clots and some countries, including Britain, have recommended that only people over a certain age get the shot.
Adam Finn, Professor of Paediatrics at Bristol University, said the jump in reported cases was expected.
[editor’s note: In a statement, the WHO reaffirmed its position that the benefits of AstraZeneca’s vaccine outweighs the risks, including the rare clotting events it has dubbed thrombosis with thrombocytopenia syndrome (TTS).]
High dose of vitamin D fails to improve condition of moderate to severe COVID-19 patients – EurekAlert
Can a high dose of vitamin D administered on admission to hospital improve the condition of patients with moderate or severe COVID-19? The answer is no, according to a Brazilian study published in the Journal of the American Medical Association (JAMA).
The article reports a randomized, double-blind, placebo-controlled clinical trial, the kind of study considered the gold standard to evaluate drug efficacy. It was conducted with FAPESP’s support by researchers at the University of Sao Paulo’s Medical School (FM-USP), who recruited 240 patients treated at Hospital das Clinicas (HC), the hospital complex run by FM-USP, and the Ibirapuera field hospital in Sao Paulo City in June-August 2020.
“In vitro studies or trials with animals had previously shown that in certain situations vitamin D and its metabolites can have anti-inflammatory and anti-microbial effects, as well as modulating the immune response. We decided to investigate whether a high dose of the substance could have a protective effect in the context of an acute viral infection, reducing either the inflammation or the viral load,” Rosa Pereira, principal investigator for the project, told Agencia FAPESP.
Only one vaccine is OK for older teens. It’s also the hardest to manage in rural America. – News-Medical
As states expand covid-19 vaccine eligibility to allow shots for 16- and 17-year-olds, teens in rural America may have trouble getting them.
Of the three vaccines authorized in the U.S., currently only one can go to that age group: the Pfizer-BioNTech shot. That vaccine comes in 1,170-dose packages at minimum and expires after five days in a fridge, meaning too many doses on too tight a deadline for many rural communities to manage.
“We’re still trying to get people to accept the vaccine,” said Aurelia Jones-Taylor, CEO of Aaron E. Henry Community Health Services Center, which serves remote regions of the Mississippi Delta. “If we have to race to give out 1,100 doses in five days, that’s untenable.”
Some health experts say vaccinating children – more than a fifth of the nation’s population – is key to ending the pandemic. In the meantime, pressure is mounting to get vaccines out as health officials flag more surges of cases, this time with more contagious variants that seem to affect kids more than the initial virus strain that coursed through the U.S.
“The infection can continue to spread until we get everyone in the population vaccinated, and that includes younger individuals,” said Gypsyamber D’Souza, an epidemiologist with Johns Hopkins Bloomberg School of Public Health.
The logistical challenges of eventually getting the shots to rural kids of all ages will likely continue, at least in the short term. That’s because the companies behind the sole vaccine with approval for 16- and 17-year-olds, Pfizer and BioNTech, have also been the first to seek federal approval to vaccinate younger ages after a trial showed the vaccine was effective in kids 12 through 15 years old. Pfizer spokesperson Steve Danehy said the company hopes to win regulatory approval for that age group before the start of the next school year.
Can We Get to ‘COVID Zero’? Experts Predict the Next 8 Months – Medscape
COVID-19 is likely to follow a seasonal pattern – similar to some other respiratory viruses – with fewer cases come summer 2021 followed by a jump next winter, experts predicted in a Thursday briefing.
If that pattern holds, it could mean a need to reinforce the mask-wearing message as the weather gets colder and people once again congregate indoors.
“Right now, we are projecting the United States all the way to August 1 [will have] 619,000 deaths from COVID-19, with 4.7 million globally,” said Ali H. Mokdad, PhD, professor of health metrics sciences at the Institute for Health Metrics and Evaluation (IHME) at the University of Washington in Seattle, during today’s media briefing sponsored by the Infectious Diseases Society of America (IDSA) and IHME.
The encouraging news is the vaccines appear to be working and more Americans are getting them. “If you look at the data for these vaccines, they are extremely safe, they are extremely efficacious, and they make you basically impervious – for the most part – to getting serious disease, hospitalization, or death,” said Amesh Adalja, MD, senior scholar at Johns Hopkins University Center for Health Security in Baltimore.
Furthermore, the US Food and Drug Administration (FDA) is likely to approve emergency use authorization (EUA) among teenagers 12 to 15 years old “imminently,” thereby expanding the pool of people potentially protected by vaccines.
Such authorization could help with overall public health efforts. “That’s simply a mathematical formula,” Adalja said. “The more people that are vaccinated, including children, the quicker we’ll get to herd immunity.”
In addition, with lower case numbers expected this summer, herd immunity might become more achievable, said Mokdad, who is also chief strategy officer for population health at the University of Washington.
As important as herd immunity is, so-called decoupling is “more important to me,” Adalja said. Decoupling refers to separating infections from the more severe outcomes, so people who get COVID-19 are less likely to need hospitalization or die from it.
MIT researchers: Risk of contracting COVID-19 indoors the same at 6ft and 60ft – The Hill
The risk of contracting COVID-19 indoors is the same when socially distanced 6 feet apart and 60 feet apart, researchers at the Massachusetts Institute of Technology (MIT) say.
The study, published in the Proceedings of the National Academy of Sciences of the United States of America earlier this month, argues that there isn’t much benefit to distancing 6 feet apart.
Ideas about coronavirus transmission have changed since the beginning of the pandemic. At the start of the global outbreak, scientists and medical professional believed that hand-washing after touching surfaces was the leading cause of transmission. Experts now say the virus is transmitted through droplets released when people talk, sneeze and cough.
Professor Martin Bazant, who teaches chemical engineering and applied mathematics at MIT, told CNBC that the rule “really has no physical basis because the air a person is breathing while wearing a mask tends to rise and comes down elsewhere in the room so you’re more exposed to the average background than you are to a person at a distance.”
Bazant and MIT applied mathematics professor John Bush created a model to calculate exposure risk to COVID-19 in an indoor setting based on the amount of time indoors, air filtration, immunizations, variants and respiratory activity like breathing.
They say the most important factor is the amount of time spent indoors rather than how far apart people stand from one another.
The following are foreign headlines with hyperlinks to the posts
Japan declared a third state of emergency Friday, which will last until May 11 to discourage holiday traveling. The Olympics committee reaffirmed its determination to hold the summer games.
Canada is banning all flights from India, as well as Pakistan, for 30 days in the midst of the countries’ alarming case rates.
Zydus Cadila’s Virafin has been granted emergency use authorisation (EUA) in India for treatment of moderate cases of Covid-19 by the Drugs Controller General of India (DCGI). Virafin is an antiviral drug that is subcutaneously administered. The drug, when given to Covid patients in the early stage, has shown significant clinical and virological improvement in moderate cases. According to the drug maker, patients who were treated with Virafin were tested negative within 7 days.
More than 50 vaccination sites down in Mumbai due to vaccine shortage
WHO: Worldwide COVID-19 Cases Reached New Weekly Record
Thailand Set to Run Out of ICU Beds in 19 Days as COVID-19 Cases Soar
China ‘Ready’ to Help India in COVID-19 Crisis Amid U.S. Raw Materials Ban
Millions go hungry as Covid continues to ravage Brazil
Brazil’s Sao Paulo state reports more than 20% decrease in weekly Covid-19 deaths
Germany’s controversial ’emergency brake’ law will close most of the country from Saturday
The following additional national and state headlines with hyperlinks to the posts
With apparently few new cases of vaccine-induced immune thrombotic thrombocytopenia, U.S. officials appear ready to lift the pause on Johnson & Johnson’s vaccine, though potentially with restrictions.
US has more than 9 million Johnson & Johnson doses ready to go if pause lifts
Nearly 80 Iowa prisoners were injected with six-times the normal dose of the Pfizer COVID-19 vaccine, though none required outside medical attention.
The newly discovered Texas SARS-CoV-2 variant, BV-1 (named for its Brazos Valley origin), showed signs of antibody-resistance, higher contagion, and more severe illness.
Available vaccines appear to be effective at neutralizing the New York variant, B.1.526.
Worldwide data on more than 2,000 pregnancies confirm that pregnant women with COVID-19 and their babies face a higher complication and mortality risk.
COVID-related hospitalizations among older folks dropped over 70% since January.
An Illinois pharmacy accidentally gave eight recipients of Moderna’s vaccine a Pfizer booster.
Diagnosed with COVID-19 between shots? NIAID Director Anthony Fauci, MD, says you’re good to get your second jab once you’re recovered and no longer contagious
The University of California and California State University systems as well as Stanford University are joining the list of schools requiring vaccination before the start of the fall semester.
COVID-19 Hospitalizations Tumble Among US Senior Citizens
CDC Director Recommends Pregnant People Receive COVID-19 Vaccines
FDA says health care workers should stop reusing N95 masks
U.S.’ Largest Maker of N95 Masks Says Company Has Millions of Unsold Units
Some mass vaccination sites in the U.S. begin to close as demand falls in many areas.
Puerto Rico sees surge in coronavirus cases, fueled by business reopenings and Spring Break.
Moderna working to have Covid-19 vaccine booster available by late summer or early fall
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
16 April 2021 ECRI’s WLI Growth Rate Marginally Declines
March 2021 Headline New Home Sales Significantly Improve
March 2021 Coincident Indices Generally Improved Month-over-Month
Warning to Readers
The amount of politically biased articles on the internet continues to increase. And studies and opinions of the experts continue to contradict other studies and expert opinions. Honestly, it is difficult to believe anything anymore.

I assemble this coronavirus update daily – sifting through the posts on the internet. I try to avoid politically slanted posts (mostly from CNN, New York Times, and the Washington Post) and can usually find unslanted posts on that subject from other sources on the internet. I wait to publish posts on subjects that I cannot validate across several sources. But after all this extra work, I do not know if I have conveyed the REAL facts. It is my job to provide information so that you have the facts necessary – and then it is up to readers to draw conclusions.
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19 when recovering from COVID-19. Herd immunity does not look like an option without immunization although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a significantly higher death rate as there is relatively few hospitalizations and deaths in younger age groups..
- There are at least 8 strains of the coronavirus. California and New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
What we do or do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work. Unfortunately, early in the pandemic, many health experts – in the U.S. and around the world – decided that the public could not be trusted to hear the truth about masks. Instead, the experts spread a misleading message, discouraging the use of masks.
- Current thinking is that we develop at least 5 months of immunity from further COVID infection.
- The Moderna and Pfizer vaccines have an effectiveness rate of about 95 percent after two doses. That is on par with the vaccines for chickenpox and measles. The 95 percent number understates the effectivenessas it counts anyone who came down with a mild case of Covid-19 as a failure. But turning Covid into a typical flu – as the vaccines evidently did for most of the remaining 5 percent – is actually a success. Of the 32,000 people who received the Moderna or Pfizer vaccine in a research trial, only one contracted a severe Covid case.
- To what degree do people who never develop symptoms contribute to transmission? Research early in the pandemic suggested that the rate of asymptomatic infections could be as high as 81%. But a meta-analysis, which included 13 studies involving 21,708 people, calculated the rate of asymptomatic presentation to be 17%.
- The accuracy of rapid testing is questioned – and the more accurate test results are not being given in a timely manner.
- Can children widely spread coronavirus? [current thinking is that they are a minor source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- Air conditioning contributes to the pandemic spread.
- It appears that there is increased risk of infection and mortality for those living in larger occupancy households.
- Male patients have almost three times the odds of requiring intensive treatment unit (ITU) admission compared to females.
- Outdoor activities seem to be a lower risk than indoor activities.
Treatments with solid scientific support:
- Dexamethasone
- Proning, or turning someone on their stomach
- Remdesivir
- Baricitinib
Treatments with potential but limited evidence:
- ECMO, or extracorporeal membrane oxygenation
- fluvoxamine
- Cyclosporine
- Famotidine
- Intravenous immunoglobulin
- Ivermectin
- Interferons
Drugs shown to be ineffective:
- The combination of lopinavir-ritonavir
- Hydroxychloroquine
- Insulin
- High dose zinc and vitamin C
- Convalescent plasma
- Monoclonal antibodies
- Tocilizumab
- Anti-coagulants
- A current scientific understanding of the way the coronavirus works can be found [here].
There is now a vaccine available – the questions remain:
- will there be any permanent side effects that will appear months from now,
- how long immunity will last [we can currently say we do not know if it will last more than 4 months],
- there is no solid evidence yet the vaccine will block transmission
Heavy breakouts of coronavirus have hit farmworkers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>





