Written by Steven Hansen
The U.S. new cases 7-day rolling average are 13.3 % HIGHER than the 7-day rolling average one week ago and U.S. deaths due to coronavirus are now 24.2 % LOWER than the rolling average one week ago. Today’s posts include:
- U.S. Coronavirus New Cases are 78,903
- U.S. Coronavirus deaths are at 352
- U.S. Coronavirus immunizations have been administered to 62.6 % of the population
- The 7-day rolling average rate of growth of the pandemic shows new cases worsened and deaths were little changed
- Will Vaccinated People Be More Vulnerable to Variants?
- New COVID-19 vaccine may offer broad protection from coronaviruses
- Why do so many vaccinated people remain irrationally fearful?
- WHO panel comes out against requiring vaccination proof for travel
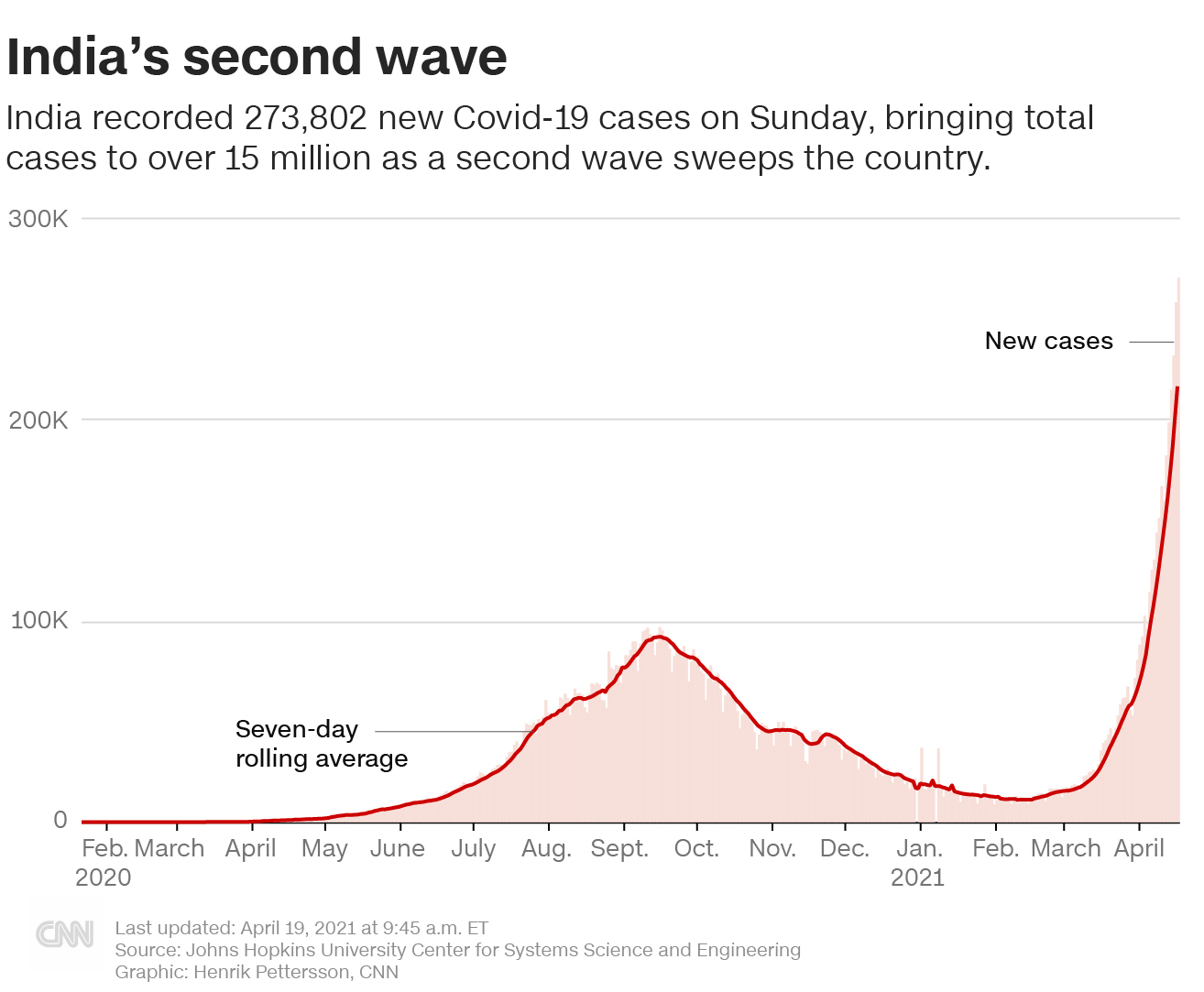
- India’s health system has collapsed
- UK human challenge trial launches to study Covid-19 reinfection
- Johnson & Johnson one-shot vaccine pause might be lifted this week, Fauci says
include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus1.htm’); ?>
Hospitalizations Are The Only Accurate Gauge
Hospitalizations historically appear to be little affected by weekends or holidays. The hospitalization growth rate trend is improving.

source: https://gis.cdc.gov/grasp/covidnet/COVID19_3.html
Historically, hospitalization growth follows new case growth by one to two weeks.
As an analyst, I use the rate of growth to determine the trend. But, the size of the pandemic is growing in terms of real numbers – and if the rate of growth does not become negative – the pandemic will overwhelm all resources.
The graph below shows the rate of growth relative to the growth a week earlier updated through today [note that negative numbers mean the rolling averages are LOWER than the rolling averages one week ago]. As one can see, the rate of growth for new cases peaked in early December 2020 for Thanksgiving, and early January 2021 for end-of-year holidays – and it now shows that the coronavirus effect is lower.

In the scheme of things, new cases decline first, followed by hospitalizations, and then deaths.
The New Variants Are The Primary Cause Of This Fourth Wave
Even with vaccinations picking up, the fourth wave is now underway.
- the more people that are vaccinated reduces the pool of people that can be infected. Today we have removed over 62 % of the population from being infected which theoretically should reduce the infection rate by 62 % [it is unproven whether the vaccines prevent a vaccinated person from being a carrier of the virus even though showing no signs]. If the vaccines are shown to stop transmission, then in theory it would reduce the infection rate by double the percent vaccinated [in this case you prevent your own infection and do not pass it along to another].
- it is also unknown what the effective rate of the current vaccines is against mutations that seem to appear almost daily. As an example, if the effective rate drops to 60%, it means the 62 % reduction in the infection rate discussed above is almost cut in half. The South African and Brazilian variant is reported somewhat immune to the current vaccines.
- In theory, the pandemic should be over immediately if everyone could be vaccinated today. The problem is that every day brings a new mutation (which would not appear if the pandemic was stopped). The longer the immunization process takes – the more ineffective the vaccine will become.
- It is not clear whether the vaccine prevents those vaccinated from spreading the virus. It seems to be well documented that it normally stops the virus from taking hold and when it does not – the infection is mild.
The real question is whether the vaccines will be mitigating this surge – and to what extent.
Coronavirus News You May Have Missed
Why do so many vaccinated people remain irrationally fearful? – New York Times
Guido Calabresi, a federal judge and Yale law professor, invented a little fable that he has been telling law students for more than three decades.
He tells the students to imagine a god coming forth to offer society a wondrous invention that would improve everyday life in almost every way. It would allow people to spend more time with friends and family, see new places and do jobs they otherwise could not do. But it would also come with a high cost. In exchange for bestowing this invention on society, the god would choose 1,000 young men and women and strike them dead.
Calabresi then asks: Would you take the deal? Almost invariably, the students say no. The professor then delivers the fable’s lesson: “What’s the difference between this and the automobile?”
In truth, automobiles kill many more than 1,000 young Americans each year; the total U.S. death toll hovers at about 40,000 annually. We accept this toll, almost unthinkingly, because vehicle crashes have always been part of our lives. We can’t fathom a world without them.
It’s a classic example of human irrationality about risk. We often underestimate large, chronic dangers, like car crashes or chemical pollution, and fixate on tiny but salient risks, like plane crashes or shark attacks.
One way for a risk to become salient is for it to be new. That’s a core idea behind Calabresi’s fable. He asks students to consider whether they would accept the cost of vehicle travel if it did not already exist. That they say no underscores the very different ways we treat new risks and enduring ones.
I have been thinking about the fable recently because of Covid-19. Covid certainly presents a salient risk: It’s a global pandemic that has upended daily life for more than a year. It has changed how we live, where we work, even what we wear on our faces. Covid feels ubiquitous.
Fortunately, it is also curable. The vaccines have nearly eliminated death, hospitalization and other serious Covid illness among people who have received shots. The vaccines have also radically reduced the chances that people contract even a mild version of Covid or can pass it on to others.
Yet many vaccinated people continue to obsess over the risks from Covid — because they are so new and salient.
To take just one example, major media outlets trumpeted new government data last week showing that 5,800 fully vaccinated Americans had contracted Covid. That may sound like a big number, but it indicates that a vaccinated person’s chances of getting Covid are about one in 11,000. The chances of a getting a version any worse than a common cold are even more remote.
But they are not zero. And they will not be zero anytime in the foreseeable future. Victory over Covid will not involve its elimination. Victory will instead mean turning it into the sort of danger that plane crashes or shark attacks present — too small to be worth reordering our lives.
That is what the vaccines do. If you’re vaccinated, Covid presents a minuscule risk to you, and you present a minuscule Covid risk to anyone else. A car trip is a bigger threat, to you and others. About 100 Americans are likely to die in car crashes today. The new federal data suggests that either zero or one vaccinated person will die today from Covid.
It’s true that experts believe vaccinated people should still sometimes wear a mask, partly because it’s a modest inconvenience that further reduces a tiny risk — and mostly because it contributes to a culture of mask wearing. It is the decent thing to do when most people still aren’t vaccinated. If you’re vaccinated, a mask is more of a symbol of solidarity than anything else.
Coming to grips with the comforting realities of post-vaccination life is going to take some time for most of us. It’s only natural that so many vaccinated people continue to harbor irrational fears. Yet slowly recognizing that irrationality will be a vital part of overcoming Covid.
“We’re not going to get to a place of zero risk,” Jennifer Nuzzo, a Johns Hopkins epidemiologist, told me during a virtual Times event last week. “I don’t think that’s the right metric for feeling like things are normal.”
After Nuzzo made that point, Dr. Ashish Jha of Brown University told us about his own struggle to return to normal. He has been fully vaccinated for almost two months, he said, and only recently decided to meet a vaccinated friend for a drink, unmasked. “It was hard — psychologically hard — for me,” Jha said.
“There are going to be some challenges to re-acclimating and re-entering,” he added. “But we’ve got to do it.”
And how did it feel in the end, I asked, to get together with his friend?
“It was awesome,” Jha said.
Johnson & Johnson one-shot vaccine pause might be lifted this week, Fauci says – AP
The pause on using the one-shot Johnson & Johnson vaccine will probably be lifted by Friday, although some restrictions may be required, Dr. Anthony Fauci said Sunday.
Fauci, director of the National Institute of Allergy and Infectious Disease, told CBS’ “Face the Nation” that “you don’t want to jump ahead of yourself and decide you know the total spectrum of this, which is one of the reasons why they paused and why hopefully by Friday we’ll know.”
Fauci, who also took his message to NBC’s “Meet the Press,” said he doubts the Food and Drug Administration and the Centers for Disease Control and Prevention will “just cancel” the J&J vaccine and continue allowing only the two-dose vaccines developed by Pfizer and Moderna.
What The CDC’s VAERS Database Reveals About “Adverse” Post-Vaccine Reactions – ZeroHedge
Data released today by the Centers for Disease Control and Prevention (CDC) on the number of injuries and deaths reported to the Vaccine Adverse Event Reporting System (VAERS) following COVID vaccines revealed reports of blood clots and other related blood disorders associated with all three vaccines approved for Emergency Use Authorization in the U.S. — Pfizer, Moderna and Johnson & Johnson (J&J). So far, only the J&J vaccine has been paused because of blood clot concerns.
VAERS is the primary mechanism for reporting adverse vaccine reactions in the U.S. Reports submitted to VAERS require further investigation before a causal relationship can be confirmed.
Every Friday, VAERS makes public all vaccine injury reports received through a specified date, usually about a week prior to the release date. Today’s data show that between Dec. 14, 2020 and April 8, a total of 68,347 total adverse events were reported to VAERS, including 2,602 deaths — an increase of 260 over the previous week — and 8,285 serious injuries, up 314 since last week.
Of the 2,602 deaths reported as of April 8, 27% occurred within 48 hours of vaccination, 19% occurred within 24 hours and 41% occurred in people who became ill within 48 hours of being vaccinated.
In the U.S., 174.9 million COVID vaccine doses had been administered as of April 8. This includes 79.6 million doses of Moderna’s vaccine, 90.3 million doses of Pfizer and 4.9 million doses of the J&J COVID vaccine.
This week’s VAERS data show:
- 19% of deaths were related to cardiac disorders.
- 55% of those who died were male, 43% were female and the remaining death reports did not include gender of the deceased.
- The average age of those who died was 77 and the youngest death was an 18-year-old. There are a few reported deaths in children under 18, but these reports contained errors.
- As of April 8, 408 pregnant women had reported adverse events related to COVID vaccines, including 114 reports of miscarriage or premature birth.
- Of the 678 cases of Bell’s Palsy reported, 59% of cases were reported after Pfizer-BioNTech vaccinations, 38% following vaccination with the Moderna vaccine and 24 cases (4%) of Bell’s Palsy were reported with J&J.
- There were 77 reports of Guillain-Barré Syndrome with 55% of cases attributed to Pfizer, 40% to Moderna and 10% to J&J.
- There were 20,021 reports of anaphylaxis with 47% of cases attributed to Pfizer’s vaccine, 46% to Moderna and 7% to J&J.
Children’s Health Defense queried the VAERS data for a series of adverse events associated with the formation of clotting disorders and other related conditions. VAERS yielded a total of 795 reports for all three vaccines from Dec. 14, 2020, through April 8.
Of the 795 cases reported, there were 400 reports attributed to Pfizer, 337 reports with Moderna and 56 reports with J&J — far more than the eight J&J cases under investigation, including the two additional cases added Wednesday.
As The Defender reported today, although the J&J and AstraZeneca COVID vaccines have been under the microscope for their potential to cause blood clots, mounting evidence suggests the Pfizer and Moderna vaccines also cause clots and related blood disorders. U.S. regulatory officials were alerted to the problem as far back as December 2020.
… Cases of fully vaccinated people getting COVID, referred to as “breakthrough” cases, continue to make news.
Calling it a “really good scenario,” the CDC yesterday reported 5,800 cases of COVID in fully vaccinated people. Of the 5,800 cases, 396 required hospitalization and 74 people died, the CDC said.
The CDC said it was “keeping a close eye” on the cases, but that breakthrough cases are to be expected. Tara Smith, a professor of epidemiology at the Kent State University College of Public Health in Ohio, told NBC News:
“This is a really good scenario, even with almost 6,000 breakthrough infections. Most of those have been mildly symptomatic or asymptomatic. That’s exactly what we were hoping for.”
Will Vaccinated People Be More Vulnerable to Variants? – Mercola
- Experts have raised warnings about the problematic history of coronavirus vaccines and their propensity to produce antibody‐dependent enhancement (ADE), which could make vaccinated individuals more susceptible to infection by SARS-CoV-2 or its variants
- An October 2020 paper stressed that “COVID‐19 vaccines designed to elicit neutralizing antibodies may sensitize vaccine recipients to more severe disease than if they were not vaccinated,” and criticized vaccine makers for not clearly informing participants in current vaccine trials of this risk
- Vaccinated individuals do appear to be more susceptible to infection by certain variants of SARS-CoV-2, although it remains to be seen whether they are more prone to serious illness
- Israeli researchers compared 400 individuals who had tested positive for the South African B.1.351 SARS-CoV-2 variant after receiving at least one dose of Pfizer’s COVID-19 vaccine against 400 unvaccinated individuals who had been infected. Among those who received two doses of the vaccine, the variant was eight times more prevalent than in unvaccinated individuals (5.4% compared to 0.7%)
- By analyzing blood samples, a second study found Pfizer’s COVID-19 vaccine was 6.8 times less effective against the South African B.1.351 variant compared to generic strains of the virus
New COVID-19 vaccine may offer broad protection from coronaviruses – EurekAlert
A COVID-19 vaccine that could provide protection against existing and future strains of the COVID-19 coronavirus, and other coronaviruses, and cost about $1 a dose has shown promising results in early animal testing.
Vaccines created by UVA Health’s Steven L. Zeichner, MD, PhD, and Virginia Tech’s Xiang-Jin Meng, MD, PhD, prevented pigs from being becoming ill with a pig model coronavirus, porcine epidemic diarrhea virus (PEDV). The vaccine was developed using an innovative approach that Zeichner says might one day open the door to a universal vaccine for coronaviruses, including coronaviruses that previously threatened pandemics or perhaps even coronaviruses that cause some cases of the common cold.
Their coronavirus vaccine offers several advantages that could overcome major obstacles to global vaccination efforts. It would be easy to store and transport, even in remote areas of the world, and could be produced in mass quantities using existing vaccine-manufacturing factories.
The UVA and Virginia Tech scientists created the vaccine using a new platform Zeichner invented to rapidly develop new vaccines. So the testing success bodes well for both the COVID-19 vaccine and Zeichner’s vaccine-development approach.
“Our new platform offers a new route to rapidly produce vaccines at very low cost that can be manufactured in existing facilities around the world, which should be particularly helpful for pandemic response,” Zeichner said.
WHO panel comes out against requiring vaccination proof for travel – The Hill
A World Health Organization (WHO) panel last week came out against any requirements that travelers show proof of their COVID-19 vaccination in order to enter certain countries, highlighting its concern that such measures would aggravate inequities.
WHO’s Emergency Committee released a statement on Monday detailing its members’ advice to WHO Director-General Tedros Adhanom Ghebreyesus, including to avoid any mandate for people to prove they took the vaccine before traveling into countries.
The panel specifically cited concerns about inequity as the vaccine remains less available in certain areas and nations, especially countries that could not afford to collect a large stockpile of vaccine doses. Others, such as the U.S., invested heavily in vaccinations and built a supply that President Biden reiterated last week is enough to vaccinate the American population.
“Do not require proof of vaccination as a condition of entry, given the limited (although growing) evidence about the performance of vaccines in reducing transmission and the persistent inequity in the global vaccine distribution,” the committee’s recommendation reads. “States Parties are strongly encouraged to acknowledge the potential for requirements of proof of vaccination to deepen inequities and promote differential freedom of movement.”
The Emergency Committee also called attention to sailors who may be blocked from crossing international borders due to requirements to prove they got the vaccine.
“Special attention should be paid to seafarers who are stranded at sea and who are stopped from crossing international borders for crew change due to travel restrictions, including requirements for proof of COVID-19 vaccination, to ensure that their human rights are respected,” the recommendation reads.
India’s health system has collapsed – Hindustan Times
“We have collapsed, Maharashtra is sinking and other states will follow.”
The starkness of these words from Dr Jalil Parkar, a top pulmonologist in Mumbai’s Lilavati Hospital, silenced me in a way that little has through 2020 and 2021, when most of my journalistic energy has been spent on reporting the Covid crisis on the ground. “This is worse than World War Two,” Parkar said, lashing out in rage and hurt at how doctors and health workers are still targeted by angry and distraught families as well as armchair commentators “who sit behind their laptops and in their ivory towers”.
Among other issues, Parkar’s reference was to a leaked video from his hospital which showed patients being treated in a lift-lobby packed with patients, and the simple-minded judgments that followed.
He is absolutely right. There will be another day to analyse the broken health care system, the woeful underspending (less than 2% of GDP) on public health, and whether Covid has pushed us towards a new policy framework.
For now, on the ground, after tracking cremation grounds and graveyards, meeting doctors and nurses inside Covid ICUs, travelling with ambulance drivers and spending hours at testing centres, I can authenticate the fact that everything — and I mean everything — is running short.
The most critical shortfall is that of oxygen. An hour from Mumbai in the Vasai-Palghar belt, eight patients died in a single day at the Vinayaka private hospital because oxygen ran out. I met the wife, son and daughter of one among them — Ram Babu, a tailor — in their tiny one-room apartment. At the centre of the room, taking pride of place, sat his sewing machine, placed on a high table, as the family sat on the cold floor, in paralysed grief.
In small residential colonies, behind closed doors, are the real people behind the clinical numbers. In the city itself, at a Covid hospital in Chembur, I saw already over-stretched ward staff, going to hunt for oxygen an hour-and-a-half away, bringing it back in tiny lorries, which they would then unload and pull up, all the while in their medical scrubs. “There is at least a 50% shortage here,” said officials at the hospital.
It is not just Mumbai. From Patna, I received a distraught call from a stranger, a young woman who identified herself as Manisha. Her father, just 53 years of age, was being asked by the Ford Hospital in the city, according to Manisha, to try and organise his own oxygen as supplies were just not reaching the facility.
At the SRV Hospital in Mumbai, Dr Rupkatha told me that not just beds but critical drugs such as Remdesivir and Tocilizumab are entirely out of stock. “Sometimes we tell patients to reach out to dealers directly, what can we do.”
Talks have begun with the military and the railways, according to Saket Tiku, the head of Indian Gas Association, on how to ferry oxygen from steel plants in the east of India to the west, where it is most critically needed. But let me translate for you in the unvarnished, chilling words of one of Maharashtra’s top Covid warriors, Dr Swaropp Hegde, what this actually means. “With not enough oxygen, we have to change our line of treatment. This will definitely mean we will see many more deaths.”
The main difference between 2020 and 2021, doctors I meet on the ground in Maharashtra say, is that younger Indians are being infected, among them children as young as five and three. The mutations may mean that instead of calling this a pandemic borne from the coronavirus, we needed to start using the word “viruses” as this strain(s) is playing out in multiple different ways.
Meanwhile, at crematoriums and graveyards, space runs short and the heart stops. In Ghatkopar, I meet a 95-year-old man in a wheelchair waiting to bid farewell to his wife. Another man, younger, angrier, shouts out. “First there was no space in hospitals, now there is no place at the shamshan ghat… Where should we go?”
India’s health system has cracked under the weight of Covid. We are in a national emergency. The images of the election rallies, the religious congregations, the farmers protests — any mass congregation — is not just idiotic, it is an insult to the doctors at the frontline who say they are “exhausted and worn out”.
More than 800 doctors have already lost their lives to Covid. We claim to respect them and salute them every day. And yet, our utter callousness and the bizarre mixed messaging from our politicians — lockdowns for citizens, rallies for netas — are a criminal affront to every health worker on duty.
As Hemant Deshmukh, dean at Mumbai’s KEM Hospital told me, “Right now, we are discussing shortage of beds and drugs and vaccines. What if we run short of doctors?”
[editor’s note: This link was sent to me from my good friend in Pune, India. THIS VIRUS WILL NOT GO AWAY WHILE HUGE CHUNKS OF THE WORLD ARE OVERWHELMED.]
UK human challenge trial launches to study Covid-19 reinfection – CNN
A year-long trial launched Monday to study how the immune system reacts in people contracting coronavirus for the second time.
Volunteers in the UK who’ve previously had Covid-19 will be deliberately infected with the virus to discover what it may mean for developing immunity.
The so-called “challenge trial” will happen under carefully controlled conditions, with treatments on hand in case volunteers becomes ill, the team at the University of Oxford said.
“Challenge studies tell us things that other studies cannot because, unlike natural infection, they are tightly controlled. When we re-infect these participants, we will know exactly how their immune system has reacted to the first Covid infection, exactly when the second infection occurs, and exactly how much virus they got,” Dr. Helen McShane, a vaccine specialist at the University of Oxford, said in a statement.
The first phase of the study, starting this month, will find the lowest dose of virus that can infect half of coronavirus survivors without causing symptoms.
Then all 64 volunteers will be infected with that dose. Their immune responses will be studied.
The following are foreign headlines with hyperlinks to the posts
Researchers at the German Primate Center (DPZ) – Leibniz Institute for Primate Research in Göttingen, Germany, have now shown that an antibody used for COVID-19 therapy is unable to effectively inhibit SARS-CoV-2 harboring a spike mutation acquired in minks. In addition, the mutation reduced the inhibition of the virus by antibodies produced in SARS-CoV-2 infected humans. These results show that SARS-CoV-2 can acquire mutations in minks that may reduce control of the virus by the human immune system (Cell Reports).
Israel, a leader in vaccination rates, has lifted its outdoor mask mandate. New daily cases are down by 98 percent since January.
India’s capital to lock down as nation’s virus cases top 15M
India faces new lockdowns plus oxygen and drug shortages as cases spiral.
India reports more than 1 million new Covid-19 cases in 5 days
Weeklong lockdown imposed in India’s capital amid coronavirus surge
All Indians 18 years and older will be eligible for Covid-19 vaccines starting May 1
France will lift some travel barriers in May
France imposes travel restrictions on four countries to keep out coronavirus variants
Mass vaccination center in France forced to close after just 58 people turn up
The situation is so bad in Brazil that the government is recommending women delay pregnancy, warning that the new P.1 variant appears to be more severe for expectant mothers than the original virus.
Countries Seek More Moderna, Pfizer COVID Shots as Concerns Mount
China’s Sinovac Vaccine 67% Effective for Symptomatic Infection
Hong Kong temporarily bans flights from India, Pakistan and the Philippines
Families are reunited as Australia and New Zealand begin their travel bubble.
Greece relaxes some quarantine rules as it prepares to welcome back tourists.
Global Covid-19 cases increase for eighth week in a row, WHO chief says
BioNTech/Pfizer agree to supply extra 100 million doses to EU
Germany’s vaccine rollout accelerates
The following additional national and state headlines with hyperlinks to the posts
The race to untangle the secrets of rare, severe blood clots after Johnson & Johnson vaccination
More than half of U.S. adults have received at least one vaccine dose.
Historic Oil Glut Amassed During the Pandemic Has Almost Gone
CDC officials are sounding the alarm on fake COVID-19 vaccination cards, as blank cards are popping up on sites like eBay left and right.
An Arab-American social service group has set up a late-night vaccine clinic in Michigan that aims to help Muslims get vaccinated during Ramadan.
Pandemic eviction bans found to protect entire communities from COVID-19 spread
Overwhelming evidence SARS-CoV-2 is airborne
A new study, published online in the journal Drug Development Research, describes the potential for the use of the plant molecule isorhamnetin in the management of COVID.
Biden Administration to Invest $1.7 B to Fight COVID-19 Variants
Watchdog report faults chaotic and unsafe response to early pandemic overseas evacuations
Walgreens Injects People With Saline Rather Than COVID Vaccine in Mix-Up
Some in New York got too much unemployment money and may have to give it back, the state says.
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
The Evolving Link Between Oil Prices And U.S. Consumer Spending
An Asynchronous And Divergent Recovery May Put Financial Stability At Risk
Fueled By Stimulus Checks, U.S. Retail Sales Soar
Warning to Readers
The amount of politically biased articles on the internet continues to increase. And studies and opinions of the experts continue to contradict other studies and expert opinions. Honestly, it is difficult to believe anything anymore.

I assemble this coronavirus update daily – sifting through the posts on the internet. I try to avoid politically slanted posts (mostly from CNN, New York Times, and the Washington Post) and can usually find unslanted posts on that subject from other sources on the internet. I wait to publish posts on subjects that I cannot validate across several sources. But after all this extra work, I do not know if I have conveyed the REAL facts. It is my job to provide information so that you have the facts necessary – and then it is up to readers to draw conclusions.
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19 when recovering from COVID-19. Herd immunity does not look like an option without immunization although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a significantly higher death rate as there is relatively few hospitalizations and deaths in younger age groups..
- There are at least 8 strains of the coronavirus. California and New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
What we do or do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work. Unfortunately, early in the pandemic, many health experts — in the U.S. and around the world — decided that the public could not be trusted to hear the truth about masks. Instead, the experts spread a misleading message, discouraging the use of masks.
- Current thinking is that we develop at least 5 months of immunity from further COVID infection.
- The Moderna and Pfizer vaccines have an effectiveness rate of about 95 percent after two doses. That is on par with the vaccines for chickenpox and measles. The 95 percent number understates the effectivenessas it counts anyone who came down with a mild case of Covid-19 as a failure. But turning Covid into a typical flu — as the vaccines evidently did for most of the remaining 5 percent — is actually a success. Of the 32,000 people who received the Moderna or Pfizer vaccine in a research trial, only one contracted a severe Covid case.
- To what degree do people who never develop symptoms contribute to transmission? Research early in the pandemic suggested that the rate of asymptomatic infections could be as high as 81%. But a meta-analysis, which included 13 studies involving 21,708 people, calculated the rate of asymptomatic presentation to be 17%.
- The accuracy of rapid testing is questioned – and the more accurate test results are not being given in a timely manner.
- Can children widely spread coronavirus? [current thinking is that they are a minor source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- Air conditioning contributes to the pandemic spread.
- It appears that there is increased risk of infection and mortality for those living in larger occupancy households.
- Male patients have almost three times the odds of requiring intensive treatment unit (ITU) admission compared to females.
- Outdoor activities seem to be a lower risk than indoor activities.
Treatments with solid scientific support:
- Dexamethasone
- Proning, or turning someone on their stomach
- Remdesivir
- Baricitinib
Treatments with potential but limited evidence:
- ECMO, or extracorporeal membrane oxygenation
- fluvoxamine
- Cyclosporine
- Famotidine
- Intravenous immunoglobulin
- Ivermectin
- Interferons
Drugs shown to be ineffective:
- The combination of lopinavir-ritonavir
- Hydroxychloroquine
- Insulin
- High dose zinc and vitamin C
- Convalescent plasma
- Monoclonal antibodies
- Tocilizumab
- Anti-coagulants
- A current scientific understanding of the way the coronavirus works can be found [here].
There is now a vaccine available – the questions remain:
- will there be any permanent side effects that will appear months from now,
- how long immunity will last [we can currently say we do not know if it will last more than 4 months],
- there is no solid evidence yet the vaccine will block transmission
Heavy breakouts of coronavirus have hit farmworkers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>





