Written by Steven Hansen
The U.S. new cases 7-day rolling average are 1.8 % HIGHER than the 7-day rolling average one week ago and U.S. deaths due to coronavirus are now 18.7 % LOWER than the rolling average one week ago. Today’s posts include:
- U.S. Coronavirus New Cases are 73,200
- U.S. Coronavirus deaths are at 992
- U.S. Coronavirus immunizations have been administered to 51.3 % of the population
- The 7-day rolling average rate of growth of the pandemic shows new cases worsened and deaths worsened
- Leaky gut and microbial dysbiosis could contribute to cytokine storm in severely ill COVID-19 cases
- Skin Reactions to COVID Vaccines Aren’t Dangerous, Study Says
- Pennsylvania attorney general warns of ‘dangerous’ market for false vaccination cards
- Rise of coronavirus variants will define the next phase of the pandemic in the U.S.
- Parasite drug as covid-19 treatment, but skeptics call it the ‘new hydroxychloroquine’
- More than half of UK positive cases asymptomatic
- European Countries May Have to Mix COVID-19 Shots Amid AstraZeneca Crisis
- Kick U.S. Kids to the Back of the Global Vax Line
- A dwindling need for office space could trounce building owners and cities even after the pandemic

include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus1.htm’); ?>
Hospitalizations Are The Only Accurate Gauge
Hospitalizations historically appear to be little affected by weekends or holidays. The hospitalization growth rate trend is improving.

source: https://gis.cdc.gov/grasp/covidnet/COVID19_3.html
Historically, hospitalization growth follows new case growth by one to two weeks.
As an analyst, I use the rate of growth to determine the trend. But, the size of the pandemic is growing in terms of real numbers – and if the rate of growth does not become negative – the pandemic will overwhelm all resources.
The graph below shows the rate of growth relative to the growth a week earlier updated through today [note that negative numbers mean the rolling averages are LOWER than the rolling averages one week ago]. As one can see, the rate of growth for new cases peaked in early December 2020 for Thanksgiving, and early January 2021 for end-of-year holidays – and it now shows that the coronavirus effect is now shrinking.

In the scheme of things, new cases decline first, followed by hospitalizations, and then deaths.
The New Variants Are The Primary Cause Of This Fourth Wave
Even with vaccinations picking up, the fourth wave is now underway.
- the more people that are vaccinated reduces the pool of people that can be infected. Today we have removed over 51 % of the population from being infected which theoretically should reduce the infection rate by 51 % [it is unproven whether the vaccines prevent a vaccinated person from being a carrier of the virus even though showing no signs]. If the vaccines are shown to stop transmission, then in theory it would reduce the infection rate by double the percent vaccinated [in this case you prevent your own infection and do not pass it along to another].
- it is also unknown what the effective rate of the current vaccines is against mutations that seem to appear almost daily. As an example, if the effective rate drops to 60%, it means the 51 % reduction in the infection rate discussed above is almost cut in half. The South African and Brazilian variant is reported somewhat immune to the current vaccines.
- The pandemic should be over immediately if everyone could be vaccinated today. The problem is that every day brings a new mutation (which would not appear if the pandemic was stopped). The longer the immunization process takes – the more ineffective the vaccine will become.
- It is not clear whether the vaccine prevents those vaccinated from spreading the virus. It seems to be well documented that it normally stops the virus from taking hold and when it does not – the infection is mild.
The real question is whether the vaccines will be mitigating this surge – and to what extent.
Coronavirus News You May Have Missed
Colorado vaccine site closes early after adverse reactions to Johnson & Johnson shot – The Hill
A COVID-19 vaccination site in Colorado closed early on Wednesday after patients experienced adverse reactions to Johnson & Johnson’s one-shot vaccine.
Centura Health, which helps run the community vaccination center at Dick’s Sporting Goods Park, said in a statement posted to Twitter that 11 patients who received the vaccine experienced adverse reactions.
Only two of the patients were taken to hospitals for further observation “out of an abundance of caution.”
Centura Health said that the number of people who experienced adverse events equaled 0.62 percent of the over 1,700 people that were vaccinated at the site on Wednesday. The 640 patients who were unable to get vaccinated have been rescheduled to get vaccinated on April 11.
In a separate statement, state officials said there is no reason for others who were vaccinated at the site on Wednesday to be concerned.
“The state has no reason to believe that people who were vaccinated today at Dick’s Sporting Goods Park should be concerned,” the statement said. “Adverse reactions are typically immediate. Health care providers monitor patients for reactions after administering vaccines for at least 15 minutes after the injection (or for 30 minutes if the patient has a history of anaphylaxis) for this reason. This event is not impacting other vaccine providers.”
Florida’s Ron DeSantis Sues Federal Government Over COVID Cruise Ship Ban – Newsweek
Florida Governor Ron DeSantis announced on Thursday that he is suing the federal government over the COVID-19 cruise ship ban.
“We have tens of thousands of Floridians…throughout the state who depend on the viability of the cruise industry for their livelihoods, their jobs, and their ability to feed their families,” DeSantis said during a press conference in Port Miami. “This is something that’s being imposed, this shutdown, by the CDC [Centers for Disease Control and Prevention] and the federal government.”
DeSantis added that while the unemployment rate in Florida is below the national average, it is much higher in Miami-Dade County due to the cruise shutdown.
“So, today I am happy to announce that on behalf of the tens of thousands of Floridians who’s livelihood depends on the viability of an open cruise industry, today Florida’s fighting back,” he said. “We’re filing a lawsuit against the federal government and the CDC demanding that our cruise ship’s be reopened immediately.”
He continued: “This will be something that we believe we have every legal right to insist upon. We don’t believe the federal government has the right to mothball a major industry for over a year based on very little evidence and very little data.”
[editor’s note: also read Carnival Cancels Cruises, ‘May Have No Choice’ But to Pull Out of U.S. and Florida sues CDC to allow cruises to resume U.S. sailings, industry pushes for better treatment and Requiring vaccinations on cruises can break “logjam” with CDC, Norwegian Cruise Line CEO says]
Rise of coronavirus variants will define the next phase of the pandemic in the U.S. – Washington Post
Variants of the coronavirus are increasingly defining the next phase of the pandemic in the United States, taking hold in ever-greater numbers and eliciting pleas for a change in strategy against the outbreak, according to government officials and experts tracking developments.
The highly transmissible B.1.1.7 variant that originated in the United Kingdom now accounts for 27 percent of all cases in this country. It is the most common variant in the United States, Rochelle Walensky, director of the Centers for Disease Control and Prevention, said Wednesday — a development that officials predicted months ago. Two other variants, which took root in South Africa and Brazil and also are more transmissible, are cropping up with increasing frequency in parts of the United States.
The bottom line on all three remains positive. In laboratory tests, vaccines are just as effective against the variant identified in the United Kingdom as they are against the original strain of the virus. And there is only a modest drop-off in their effectiveness against two others.
“These variants emerged because we continued to give the virus more chance to spread,” said David D. Ho, whose lab at Columbia University is leading the research on the P. 1 variant first discovered in Brazil. “The sooner we vaccinate everyone, the faster we will contain the viral spread and reduce the chance for new variants to emerge.”
But the overall picture hides problems in some places. One or more of the variants — which also cause more severe disease than the original version of the virus — are racing through the Northeast and the Midwest. That has prompted officials in some communities to ask for more vaccine than they would receive under the government’s population-based formula. Officials in the Northwest are watching a major outbreak of the P. 1 variant in British Columbia.
Kick U.S. Kids to the Back of the Global Vax Line – MedPage
It was entirely possible that vaccinating older healthcare workers, even those with less patient contact, was preferable to vaccinating younger workers on the front lines. This is simply because the risk of bad COVID-19 outcomes grows massively with age and, simultaneously, the danger of being on the front lines has diminished. By January 2021, the risk of healthcare workers contracting SARS-CoV-2 in the hospital was drastically lower than early on in the pandemic, in part due to appropriate countermeasures deployed during the pandemic, such as ventilation and PPE. In other words, what looked like an injustice (residents come last) might actually save more lives.
But one can take this logic further: why not simply vaccinate people based on age, irrespective of occupation, a strategy closer to what the U.K. adopted? And what if we gave more people a first dose and delayed the second dose, rather than giving two doses to fewer people? Finally, if we want to prioritize frontline workers, what if we gave vaccines first to people truly working the highest-risk jobs? That isn’t resident physicians, it turns out, but cooks, people who package, agriculture workers, bakers, and construction workers. To some degree, all of these ideas might have saved more lives than what we chose to do in the U.S.
In the next couple months, the U.S. will have vaccinated every adult who wants one. What comes after this? Pfizer has released results from a randomized trial powered for immunologic endpoints that claim efficacy in 12- to 15-year-olds. At the same time, millions of elderly individuals in Africa, Asia, and South America remain unvaccinated.
The risk of dying from COVID-19 is incredibly low in children and adolescents. In 2020, the chance that a kid ages 5 to 14 would die of COVID-19 was one in a million. To put that in perspective, in a normal year, the risk a child commits suicide in this same age group is 10 times higher. In contrast, the risk of death if an 80-year-old becomes infected is as high as 20%. For outcomes besides death, one study showed that visits to the ICU from severe cases of COVID-19 or multi-inflammatory syndrome in children (MIS-C) occurs in one in 130,000 kids.
After all U.S. adults who wish to be vaccinated are vaccinated, COVID-19 hospitalizations will plummet, deaths will plummet too. Cases are more unpredictable, but it is likely they too will plummet. What should our policy be next? Should the U.S. commence vaccinating adolescents in this country? Or instead, should these limited doses be given to older individuals in other nations?
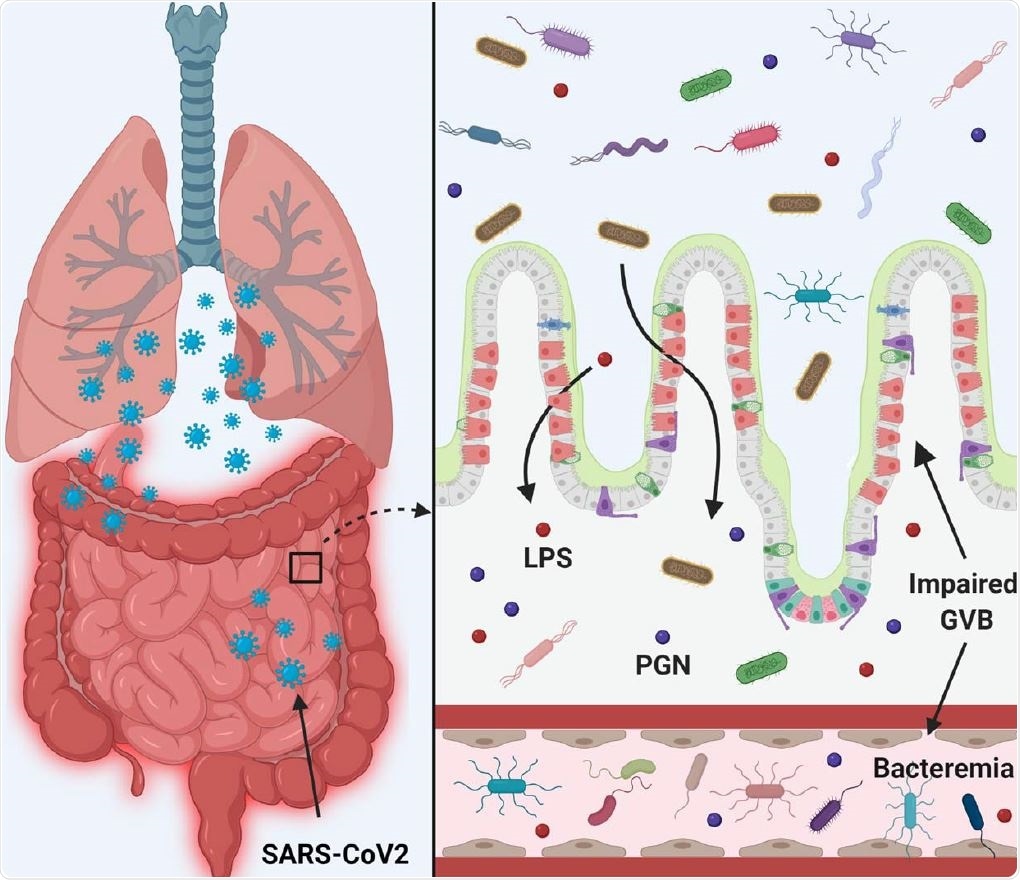
Leaky gut and microbial dysbiosis could contribute to cytokine storm in severely ill COVID-19 cases – News-Medical
As the world approaches the grim milestone of three million deaths from COVID-19 disease, a new preprint research paper posted to the bioRxiv* server shows that the presence of gut bacteria in the plasma may be an indicator of progressive disease. In patients with pre-existing comorbidities, COVID-19 is associated with more severe disease.
The gut is a well-established route of infection and target for viral damage by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the causative agent for COVID-19. This is supported by the clinical observation that about half of COVID-19 patients exhibit gastrointestinal (GI) symptoms.
Hospitalized patients with critical COVID-19 also often have gut complications. Besides the above, venous or arterial thromboembolism of the mesenteric vessels and small bowel ischemia is reported, especially in patients hospitalized for more extended periods.
SARS-CoV-2 infection disrupts the gut barrier and leads to elevation of systemic bacterial lipopolysaccharide and peptidoglycan and serves to enhance systemic inflammation. Therefore, leaky gut and microbial dysbiosis could contribute to cytokine storm in patients severely ill with COVID -19.
… The translocation of gut microbes, normally found only in feces, into the systemic circulation is a fundamental determinant of immune function and metabolism. The presence of gut microbes in plasma may trigger and also exacerbate inflammatory signaling pathways in the body.
Inflammation is key to the pathogenesis of severe and critical COVID-19. This study’s findings may support the theory that this is driven by gut bacterial movement into the body’s circulation in these patients. This, in turn, could be due to higher gut permeability because of epithelial barrier dysfunction.
Virus shedding in the feces has been found to persist for up to a month after lung symptoms resolve, indicating that viral colonization of the gut may be of longer duration than of the airways.
[editor’s note: based on this commentary, one would assume hemorrhoids would also be a problem]
Skin Reactions to COVID Vaccines Aren’t Dangerous, Study Says – Medscape
The Pfizer/BioNTech and Moderna coronavirus vaccines can cause several kinds of skin reactions, but these reactions go away quickly and aren’t dangerous, according to a study published in the Journal of the American Academy of Dermatology.
Researchers studied 414 patients with vaccine skin reactions from Dec. 24, 2020, to Feb. 14, 2021. The median age of the patients was 44, 90% were female, and 78% were white, the study says. The cases were reported by doctors including dermatologists, nurses, and other healthcare workers.
The best news is that none of the reactions were life threatening, Dr. Esther Freeman, the senior author of the study, told USA Today.
“People can get full-body rashes, and that can be surprising and a little scary, but these patients did extremely well, recovered and were able to go back and get their second dose,” said Freeman, who is director of global health dermatology at Massachusetts General Hospital.
“For people whose rashes started four or more hours after getting the vaccine, zero percent of them went on to get anaphylaxis or any other serious reaction. Zero is a nice number.”
Skin reactions can occur about a week after a shot, the study said. Any reaction — on the skin or otherwise — that occurs less than four hours after the shot may be an allergic reaction and is a cause for alarm, doctors say.
European Countries May Have to Mix COVID-19 Shots Amid AstraZeneca Crisis – Reuters
Several European countries are considering mixing up COVID-19 vaccines for citizens who received a first dose of AstraZeneca’s shot, an unprecedented move that highlights challenges for governments struggling to tame fresh rises in infections.
Vaccination programmes have been upset after a small number of reports that recipients of the AstraZeneca inoculation have suffered extremely rare blood clots, leading some countries worldwide to suspend its use out of caution.
A senior official for the European Medicines Agency (EMA) said in an interview published on Tuesday there was a link between the vaccine and rare blood clots in the brain but the possible causes were still unknown.
The EMA later said in a statement that its review of the vaccine was ongoing. It will give an update on its investigation on Wednesday afternoon.
AstraZeneca has said previously its studies have found no higher risk of clots because of the vaccine, millions of doses of which have been administered worldwide.
While many countries have resumed using the shot, some have imposed age restrictions.
In many instances, this has left officials scratching their heads over what to do for people who received a first dose of AstraZeneca but are no longer eligible under the new rules.
Pennsylvania attorney general warns of ‘dangerous’ market for false vaccination cards – The Hill
Pennsylvania Attorney General Josh Shapiro (D) is warning the public about the “dangerous” market of people selling fake vaccination cards.
“We’re seeing a huge market for these false cards online,” Shapiro said, according to The New York Times. “This is a dangerous practice that undermines public health.”
Fake vaccination cards first appeared online and picked up traction in January on platforms such as Facebook, Twitter, Shopify, eBay and Etsy.
Saoud Khalifah, the founder of Fakespot, told The New York Times that some cards are being obtained by those who don’t want to get the vaccine and others are getting the cards in order to trick pharmacies into giving them their shot.
A person will write on the fake card that they received their first coronavirus shot so a pharmacy will be obligated to give them the second dose. Two out of the three vaccines approved in the U.S. require two shots.
“We want to see them stop immediately,” Shapiro said about those selling the fake cards. “And we want to see the companies take serious and immediate action.”
The fake vaccination cards could violate federal copyright laws, state laws involving impersonation, and civil and consumer protection laws, Shapiro said.
A dwindling need for office space could trounce building owners and cities even after the pandemic. – New York Times
Businesses have discovered during the pandemic that they can function with nearly all of their workers out of the office, an arrangement that many intend to continue in some form. That could wallop the big property companies that build and own office buildings — and lead to a sharp pullback in construction, steep drops in office rents, fewer people frequenting restaurants and stores, and potentially perilous declines in the tax revenue of city governments and school districts.
In only a year, the market value of office towers in Manhattan, home to the country’s two largest central business districts, has plummeted 25 percent, according to city projections released on Wednesday. That has contributed to an estimated $1 billion drop-off in property tax revenue.
JPMorgan Chase, Ford Motor, Salesforce and Target are giving up expensive office space, and others are considering doing so. Jamie Dimon, the chief executive of JPMorgan Chase, the largest private sector employer in New York City, wrote in a letter to shareholders this week that remote work would “significantly reduce our need for real estate.” For every 100 employees, he said, the bank “may need seats for only 60 on average.”
Across the country, the vacancy rate for office buildings in cities’ downtown areas has steadily climbed over the past year to reach 16.4 percent, according to Cushman & Wakefield — the highest in about a decade. That number could climb further, even as vaccinations allow some people to go back to work, if companies keep giving up office space because of hybrid or fully remote work.
… So far, the cities with the lowest return-to-office rates are on the coasts — including New York, San Francisco and Washington — where long commutes, often on dysfunctional transit systems, are common, according to the security company Kastle Systems.
Moody’s said in March that office landlords with many buildings in coastal cities would come under the most financial pressure in the coming years.
More than half of UK positive cases asymptomatic, figures show – CNN
More than half of the people who tested positive for Covid-19 in the UK did not have symptoms, the Office for National Statistics (ONS) said Thursday in its latest Infection Survey.
“In March 2021, 47% of people testing positive for the coronavirus in the UK with a strong positive test reported symptoms and 53% did not report having any symptoms,” the ONS said.
But how did the others feel? Fatigue, headache and a cough were the most reported symptoms from people who tested positive for Covid-19. Nausea, abdominal pain and diarrhea were among the less commonly reported symptoms.
“Asymptomatic” describes a person who is infected but does not have symptoms. With Covid-19, asymptomatic carriers can still easily infect others without knowing it. So if you’re infected but don’t feel sick, you could still get others very sick.
Parasite drug as covid-19 treatment, but skeptics call it the ‘new hydroxychloroquine’ – Washington Post
… interest in ivermectin is running high, despite insufficient evidence that it works as a treatment for covid-19 and the sometimes dangerous consequences when people take the animal version. The Food and Drug Administration said at least three people were hospitalized in February after taking the veterinary formulation. It warned that high doses can cause allergic reactions, seizures, liver injury and even death.
Experts say some people are snapping up the animal drug because it is easier to obtain than the one designed for people. That formula is approved for tropical maladies and requires a prescription. And although ivermectin is touted on social media as something that could end the pandemic, it has not been cleared for use against covid-19, the disease caused by the novel coronavirus.
“It’s like the new hydroxychloroquine,” said Angela Rasmussen, a virologist at Georgetown University’s Center for Global Health Science and Security, referring to the malaria drug pushed by President Donald Trump that proved ineffective against covid-19. “It would be great if ivermectin did work — it’s been around for years and is cheap. But to my knowledge, there is no data that suggests it’s good for covid-19.”
Ivermectin is highly effective in treating devastating parasitic infections such as river blindness and is safe when used at recommended doses. In the 1970s, Japanese and U.S. scientists discovered the compound that led to its development, and in 2015 received the Nobel Prize. But against covid-19, there is “no meaningful evidence” of efficacy, according to Merck, which makes the brand-name version. And the nation’s leading organization of infectious-disease doctors recommends against using ivermectin outside of clinical trials.
But Pierre Kory, a critical-care physician, is undeterred. Kory, a co-founder of the Front Line Covid-19 Critical Care Alliance, a group of physicians and scientists from several countries, argues that studies from around the world show ivermectin is a “miracle drug” for covid-19 and should be deployed immediately. He opposes waiting for data from large randomized clinical trials to authorize its use, saying too many people are dying of covid-19.
Now, the National Institutes of Health might wade into the controversy. It is planning a randomized clinical trial to explore whether older, already approved drugs can be repurposed to reduce covid-19 symptoms, according to three individuals who spoke on the condition of anonymity because the plans have not been announced. Ivermectin is considered a top candidate for the trial, though the details are not final, the individuals said. Other possibilities are fluvoxamine, a decades-old antidepressant, and famotidine, the generic name for Pepcid, outside scientists said. The goal would be to get results within months.
The following are foreign headlines with hyperlinks to the posts
India reported a record-high spike in coronavirus infections, and the world’s largest vaccine maker, based there, went public with worries about the firm’s ability to meet demand.
Twenty-one players on the N.H.L.’s Vancouver Canucks — nearly the whole team — have tested positive.
French Open postponed by a week because of pandemic
Children and Corona: More infections than reported cases during second wave in Germany
One in ten have long-term effects 8 months following mild COVID-19
Brazil Detects First Case of South African Variant as COVID-19 Deaths Soar
Brazil’s COVID-19 death toll to surpass that of worst US wave
Iran sets record for coronavirus cases for third straight day
UK recommends limiting AstraZeneca vaccine to people over age 30
A day after European regulators described a “possible link” between AstraZeneca’s Covid-19 vaccine and rare blood clots, the vaccine faced increasing hurdles on Thursday as countries around the world move to restrict its use in younger people. The decisions are the latest setback for AstraZeneca, the company behind the world’s most widely used coronavirus vaccine.
Slovakia questions Russia’s Sputnik vaccine, saying its doses differ from a Lancet-reviewed formula.
New Zealand will suspend travel from India, the biggest coronavirus hot spot.
Piñata makers in Mexico take a hit as parties come to a standstill.
EU on track for herd immunity by mid-July, EU vaccine chief says
Rate of coronavirus infection ‘levelled off’ in England: Imperial College London
Iran tops 2 million cases as new infections double in a week
India reports more than 126,000 new Covid-19 cases in another record high
The following additional national and state headlines with hyperlinks to the posts
Raytheon Giving Employees Bonuses for Getting COVID-19 Vaccine
New York will offer one-time payments of up to $15,600 to undocumented immigrants who lost work during the pandemic and could not get unemployment benefits.
After the European Union’s drug regulator warned of a potential link between AstraZeneca’s COVID-19 injection and blood clots, authorities in Britain, Belgium and Australia all recommended against it in younger adults.
The JAK inhibitor baricitinib didn’t meet its primary endpoint in a COVID trial, aimed to determine whether it could keep hospitalized patients off respiratory support
The NIH began a clinical trial to assess safety of the Moderna and Pfizer/BioNTech vaccines in patients with severe allergies.
Akili Interactive said it has a video game in the works to treat COVID-19 “brain fog.”
A British chef has a cookbook out with “science-based” recipes for people who have lost their senses of taste and smell from lingering COVID-19.
COVID Triggers Novel Infectious Skin Condition in Teen
Hispanic immigrants of working age at highest risk of dying from COVID-19
Better masks, adequate ventilation can reduce spread of COVID-19 virus in enclosed spaces
COVID-19 antibodies persist in breast milk for months following mother’s vaccination
Autoantibodies may contribute to severe COVID-19 and potential long-COVID-19 symptoms
Authorities shut down illegal party with over 5,000 attendees in Tonto National Forest
How AstraZeneca Blood Clot Risk Compares to the Pill, Smoking, Long Flights
Idaho Becomes 3rd State to Ban ‘Vaccine Passports’, Iowa Could Be Next
Biden Suffers Reopening Setback as Fewer Students Attend School Full Time
Military vaccinations slow abroad, and the Pentagon points to a Johnson & Johnson factory error.
Scientists identify five new cases of double mutant Covid variant in California
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
03 April 2021 New York Fed Weekly Economic Index (WEI): Index Again Improved
03 April 2021 Initial Unemployment Claims Rolling Average Worsened
February 2021 Consumer Credit Shows No Year-over-Year Growth
Slow-Healing Scars: The Pandemics Legacy
What Is The Origin Of COVID-19?
Warning to Readers
The amount of politically biased articles on the internet continues to increase. And studies and opinions of the experts continue to contradict other studies and expert opinions. Honestly, it is difficult to believe anything anymore.

I assemble this coronavirus update daily – sifting through the posts on the internet. I try to avoid politically slanted posts (mostly from CNN, New York Times, and the Washington Post) and can usually find unslanted posts on that subject from other sources on the internet. I wait to publish posts on subjects that I cannot validate across several sources. But after all this extra work, I do not know if I have conveyed the REAL facts. It is my job to provide information so that you have the facts necessary – and then it is up to readers to draw conclusions.
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19 when recovering from COVID-19. Herd immunity does not look like an option without immunization although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a significantly higher death rate as there is relatively few hospitalizations and deaths in younger age groups..
- There are at least 8 strains of the coronavirus. California and New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
What we do or do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work. Unfortunately, early in the pandemic, many health experts — in the U.S. and around the world — decided that the public could not be trusted to hear the truth about masks. Instead, the experts spread a misleading message, discouraging the use of masks.
- Current thinking is that we develop at least 5 months of immunity from further COVID infection.
- The Moderna and Pfizer vaccines have an effectiveness rate of about 95 percent after two doses. That is on par with the vaccines for chickenpox and measles. The 95 percent number understates the effectivenessas it counts anyone who came down with a mild case of Covid-19 as a failure. But turning Covid into a typical flu — as the vaccines evidently did for most of the remaining 5 percent — is actually a success. Of the 32,000 people who received the Moderna or Pfizer vaccine in a research trial, only one contracted a severe Covid case.
- To what degree do people who never develop symptoms contribute to transmission? Research early in the pandemic suggested that the rate of asymptomatic infections could be as high as 81%. But a meta-analysis, which included 13 studies involving 21,708 people, calculated the rate of asymptomatic presentation to be 17%.
- The accuracy of rapid testing is questioned – and the more accurate test results are not being given in a timely manner.
- Can children widely spread coronavirus? [current thinking is that they are a minor source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- Air conditioning contributes to the pandemic spread.
- It appears that there is increased risk of infection and mortality for those living in larger occupancy households.
- Male patients have almost three times the odds of requiring intensive treatment unit (ITU) admission compared to females.
- Outdoor activities seem to be a lower risk than indoor activities.
Treatments with solid scientific support:
- Dexamethasone
- Proning, or turning someone on their stomach
- Remdesivir
- Baricitinib
Treatments with potential but limited evidence:
- ECMO, or extracorporeal membrane oxygenation
- fluvoxamine
- Cyclosporine
- Famotidine
- Intravenous immunoglobulin
- Ivermectin
- Interferons
Drugs shown to be ineffective:
- The combination of lopinavir-ritonavir
- Hydroxychloroquine
- Insulin
- High dose zinc and vitamin C
- Convalescent plasma
- Monoclonal antibodies
- Tocilizumab
- Anti-coagulants
- A current scientific understanding of the way the coronavirus works can be found [here].
There is now a vaccine available – the questions remain:
- will there be any permanent side effects that will appear months from now,
- how long immunity will last [we can currently say we do not know if it will last more than 4 months],
- there is no solid evidence yet the vaccine will block transmission
Heavy breakouts of coronavirus have hit farmworkers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>





