Written by Steven Hansen
The U.S. new cases 7-day rolling average are 6.5 % LOWER than the 7-day rolling average one week ago. U.S. hospitalizations due to COVID-19 are now 13.2 % LOWER than the rolling average one week ago. U.S. deaths due to coronavirus are now 1.7 % LOWER than the rolling average one week ago. Today’s posts include:
- U.S. Coronavirus New Cases are 73,006
- U.S. Coronavirus hospitalizations are at 51,116
- U.S. Coronavirus deaths are at 2,151
- U.S. Coronavirus immunizations have been administered to 21.7 % of the population
- The 7-day rolling average rate of growth of the pandemic shows new cases improved, hospitalizations worsened, and deaths worsened [note: this is a sign of trend reversal – could the new variants be impacting COVID case growth?>
- Here is the Johnson & Johnson vaccine distribution plan that local health officials expect to see
- These 7 States Are On The Verge Of Herd Immunity
- COVID-19 Vaccination Linked to Less Mechanical Ventilation
- Coronavirus in the U.S.: Where cases are growing and declining
- With Variants, COVID-19 Race Becomes a Sprint
- Open a window to reduce virus spread, CDC tells schools in new ventilation recommendations

The recent worsening of the trendlines for new cases is behind us which was attributed to going back to college/university, cooler weather causing more indoor activities, mutation of the virus, fatigue from wearing masks / social distancing, holiday activities, and some loosening of regulations designed to slow the coronavirus spread.
My continuing advice is to continue to wash your hands (especially after using the toilet as COVID first sheds in your stool), putting down the toilet seat (as flushing the toilet releases a plume), wear masks, avoid crowds, and maintain social distancing. No handwashing, mask, or social distancing will guarantee you do not get infected – but it sure as hell lowers the risk in all situations – and the evidence to-date shows a lower severity of COVID-19. In addition, certain activities are believed to carry higher risk – like being inside in air conditioning and removing your mask (such as restaurants, around your children/grandchildren, bars, and gyms). It is all about viral load – and outdoor activities are generally safe if you can maintain social distance. Finally, studies show eating right (making sure you are supporting your immune system) and adequate sleep increase your ability to fight off COVID.
include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus1.htm’); ?>
Hospitalizations Are The Only Accurate Gauge As Reporting Is Not Affected By Holidays
The 4 day Thanksgiving holiday period put the first wobble in the trends. Over weekends and holidays, the number of new cases and deaths decline. Over weekends, this is not a problem for week-over-week rolling averages as weekends are compared against the previous weekend. But when a holiday falls within a working week, a non-working day is compared to a working day which causes havok in the trends.
However, hospitalizations historically appear to be little affected by weekends or holidays – the daily counts do not vary significantly from day-to-day.
The hospitalization growth rate trend is improving.

For the Thanksgiving and the end of the year holiday period – roughly, it seems each appears to have added around 5 % to the rate of growth of new cases, hospitalizations, and deaths.
Historically, hospitalization growth follows new case growth by one to two weeks.
As an analyst, I use the rate of growth to determine the trend. But, the size of the pandemic is growing in terms of real numbers – and if the rate of growth does not become negative – the pandemic will overwhelm all resources.
The graph below shows the rate of growth relative to the growth a week earlier updated through today [note that negative numbers mean the rolling averages are LOWER than the rolling averages one week ago]. As one can see, the rate of growth for new cases peaked in early December 2020 for Thanksgiving, and early January 2021 for end of year holidays – and the rate of growth is now contracting.

In the scheme of things, new cases decline first, followed by hospitalizations, and then deaths.
It is up to each of our readers to protect themselves and others by washing hands, wearing a mask, avoiding crowds, and maintaining social distancing.
Will The New Variants Cause The Next Spike?
Maybe and maybe not. It all depends on vaccinations:
- the more people that are vaccinated reduces the pool of people that can be infected. Today we have removed over 21 % of the population from being infected which theoretically should reduce the infection rate by 21 % [it is unstudied whether the vaccines prevent a vaccinated person from being a carrier of the virus even though showing no signs]. If the vaccines are shown to stop transmission, then in theory it would reduce the infection rate by double the percent vaccinated [in this case you prevent your own infection and do not pass it along to another].
- it is also unknown what the effective rate of the current vaccines is against mutations that seem to appear almost daily. As an example, if the effective rate drops to 60%, it means the 21 % reduction in the infection rate discussed above is almost cut in half. The South African and Brazilian variant is somewhat immune to the current vaccines.
- The pandemic should be over immediately if everyone could be vaccinated today. The problem is that every day brings a new mutation (which would not appear if the pandemic was stopped). The longer the immunization process takes – the more ineffective the vaccine will become.
- It is not clear whether the vaccine prevents those vaccinated from spreading the virus. It seems to be well documented that it normally stops the virus from taking hold and when it does not – the infection is mild.
Coronavirus News You May Have Missed
J&J COVID Vaccine Gets Green Light from FDA Panel – MedPage
An FDA advisory committee voted unanimously Friday to recommend the Johnson & Johnson COVID-19 vaccine (Ad26.COV2.S) for use in adults 18 and older.
Based on the totality of scientific evidence available, the FDA’s Vaccines and Related Biological Products Advisory Committee (VRBPAC) voted 22-0 that benefits of the vaccine “outweigh its risks for use in individuals 18 years of age and older,” so the vaccine should qualify for FDA emergency use authorization (EUA). Most members focused on the importance of getting out another vaccine against the virus, given the rising number of variants threatening to curtail progress against the pandemic.
“This was a relatively easy call,” said Eric Rubin, MD, PhD, of Harvard T.H. Chan School of Public Health in Boston, and editor-in-chief of the New England Journal of Medicine. “It’s a bit challenging to understand how to use it clinically right now, but it still has a place.”
Part of the confusion may have arisen from the presentation from Johnson & Johnson’s Janssen Biotech division, which mentioned a two-dose study currently in progress.
VRBPAC acting chair Arnold Monto, MD, of the University of Michigan, implied that was a question for CDC’s Advisory Committee on Immunization Practices, “especially if the two-dose formulation … appears to be more efficacious.” The FDA panel could only review the vaccine as a one-dose regimen at the Friday meeting, since that was what Johnson & Johnson had applied for.
FDA staff confirmed if an EUA was issued, and two doses subsequently prove to be more effective, the authorization could be amended.
Data supporting the current EUA application (the same as presented in pre-meeting briefing documents) were primarily from the phase III multi-national randomized, placebo-controlled trial dubbed ENSEMBLE by Johnson and Johnson, and sponsored in part by the National Institute of Allergy and Infectious Diseases. They showed 66.9% efficacy (95% CI 59.0%-73.4%) against moderate to severe COVID-19 at 14 days and 66.1% (95% CI 55.0-74.8%) at 28 days following vaccination. Vaccine efficacy in the U.S., which was 74.4% at 14 days following vaccination and 72% at 28 days following vaccination.
While the vaccine was mostly effective across demographic groups, FDA technical staff noted efficacy was lower among adults 60 and older with comorbidities versus healthier seniors. The two medically attended COVID-19 cases in the vaccine group were among older adults with comorbidities.
Peter Marks, MD, PhD, director of FDA’s Center for Biologics Evaluation and Research, jumped into the discussion, asking whether the committee was comfortable with the reduced efficacy in that group, as “people may be looking at that with a lot of scrutiny.” However, panel members demurred, appearing satisfied with the explanation that the follow-up period was shorter for those participants and as more cases accrued, the product’s efficacy for that subgroup would become clearer.
Another issue for the committee was how the manufacturer defined moderate to severe COVID-19, with David Kim, MD, an HHS official, taking up the issue initially raised in the open public hearing. He pointed out that the manufacturer defined “moderate” COVID-19 as two symptoms plus a positive PCR test, with “mild” COVID as one symptom plus a positive PCR test, leading to “a total lack of mild COVID cases in the study.”
Kim said the manufacturer needed to be “consistent” with definitions currently used by FDA, CDC and the other two vaccine manufacturers, and state their claim of 67% vaccine effectiveness “applies to symptomatic COVID.”
Efficacy against severe COVID-19 for the entire cohort was 76.7% (95% CI 54.6%-89.1%) 14 days after vaccination and 85.4% (95% CI 54.2%-96.9%) at least 28 days after vaccination. A post-hoc analysis found two COVID-related hospitalizations in the vaccine group and 29 in the placebo group after 14 days, with 0 and 16 cases after 28 days, respectively.
Here is the Johnson & Johnson vaccine distribution plan that local health officials expect to see – CNN
State and local officials got draft plans for how the US Centers for Disease Control and Prevention will distribute Johnson & Johnson’s Covid-19 vaccine Friday, once it gets emergency use authorization from the US Food and Drug Administration.
They can start ordering vaccines as soon as Sunday, said an official who has seen the plans.
FDA advisers recommended EUA on Friday and the FDA has said it will move ahead quickly with the decision.
On Sunday, the CDC’s Advisory Committee on Immunization Practices (ACIP) will meet to discuss and vote on recommendations for the vaccine. But the CDC is ready to go and has put its plans into Tiberius, the federal government’s software platform used for distributing Covid-19 vaccines.
“In anticipation of everything going as planned on Sunday with the ACIP group, allocations have already been put into Tiberius for shipments next week,” said Lori Tremmel Freeman, chief executive officer of the National Association of County and City Health Officials.
She said 3.9 million doses will be available for ordering right away. “About 2.8 million will go to state and local jurisdictions; 800,000 to the retail pharmacy program,” Freeman told CNN. She added that 70,000 will go to community vaccine centers and 90,000 to the federally qualified health centers. Ordering can begin on Sunday.
“For the initial week of distribution, orders will arrive one to two days after (they are) placed, and orders will be delivered by UPS or FedEx,” Freeman said. “The manufacturer information should be live after the EUA release, assuming that gets done tomorrow.”
Freeman said the 3.9 million doses from Johnson & Johnson could add at least 25% more Covid-19 vaccination capacity for states — since currently 14.5 million doses are allocated per week to states, tribes, and territories and 3.9 million represents about 26.9% of that.
COVID-19 Vaccination Linked to Less Mechanical Ventilation – Medscape
Immunization of people 70 and older with the Pfizer/BioNTech COVID-19 vaccine in Israel was associated with a precipitous drop in need for mechanical ventilation, new evidence reveals.
Compared with residents younger than 50 — so far vaccinated at lower rates than the higher-risk older people — Israelis 70 and older were 67% less likely to require mechanical ventilation for SARS-CoV-2 infection in February 2021 compared with October-December 2020.
“This study provides preliminary evidence at the population level for the reduction in risk for severe COVID-19, as manifested by need for mechanical ventilation, after vaccination with the Pfizer-BioNTech COVID-19 vaccine,” lead author Ehud Rinott, Department of Public Health, Faculty of Health Sciences, Ben-Gurion University of the Negev in Beer-Sheva, Israel, and colleagues write.
The study was reported online February 26, 2021, in Morbidity and Mortality Weekly Report (MMWR).
The progress of COVID-19 vaccination across Israel presents researchers with a unique opportunity to study effectiveness on a population level. In this study, 84% of residents 70 and older received two-dose vaccinations. In contrast, only 10% of people in Israel younger than 50 received the same vaccine coverage.
Along with senior author Yair Lewis, MD, PhD, and coauthor Ilan Youngster, MD, Rinott compared mechanical ventilation rates between October 2, 2020, and February 9, 2021. They found that the ratio of people 70 and older compared with those younger than 50 requiring mechanical ventilation changed from 5.8:1 to 1.9:1 between these periods. This translates to the 67% decrease.
The study offers a “real-world” look at vaccination effectiveness, adding to more controlled evidence from clinical trials. “Achieving high vaccination coverage through intensive vaccination campaigns has the potential to substantially reduce COVID-19-associated morbidity and mortality,” the researchers write.
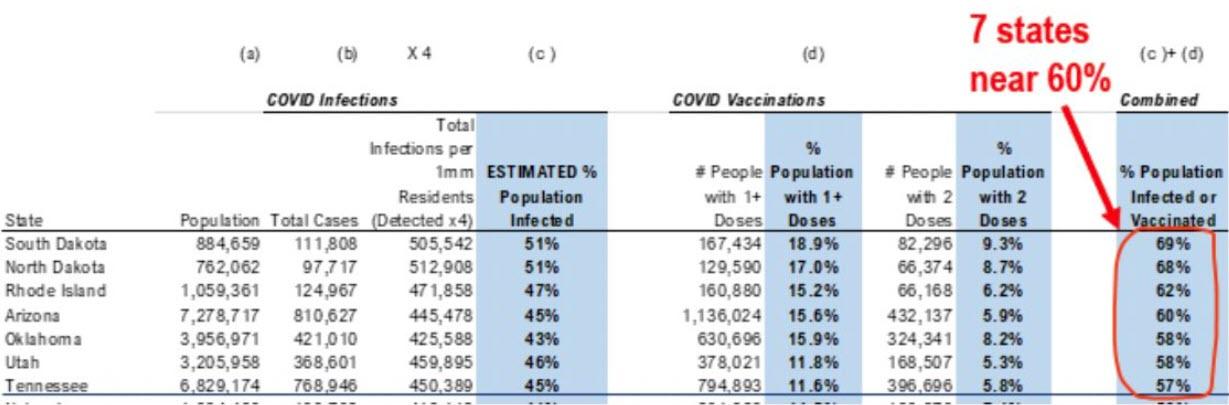
These 7 States Are On The Verge Of Herd Immunity – ZeroHedge
Nothing seems to scare the establishment more than a return to ‘normal’. And by ‘normal’, we mean a return to an environment outside of the tyrannical control of career politicians and bureaucrats who have got a taste for this ‘being king’ stuff and know that anyone who questions their edicts will be ‘canceled’ by their Covidian cultists.
So, a week after Johns Hopkins surgeon, Dr. Marty Makary, penned an Op-ed in the WSJ saying that we will have herd immunity by April… and was instantly disavowed as ‘dangerous’, some awkward ‘facts’ and ‘science’ have been dropped by none other than FundStrat’s Tom Lee.
“…cumulatively and slowly, the US is seeing more states reach that combined level of vaccinations + infections approach what is seen as herd immunity.”
So far, South Dakota, North Dakota, Rhode Island, Arizona, Oklahoma, Utah, and Tennessee are the nearest.
Lee’s “math” – which we also know is racist – appears to fit with Makary’s arguments for why the recent plunge in cases, hospitalizations, and deaths is not policy-related (no matter how much the politicians and their media lackeys push that narrative):
“…the consistent and rapid decline in daily cases since Jan. 8 can be explained only by natural immunity. Behavior didn’t suddenly improve over the holidays; Americans traveled more over Christmas than they had since March. Vaccines also don’t explain the steep decline in January. Vaccination rates were low and they take weeks to kick in.”
“Experts should level with the public about the good news…” exclaims Makary, and this data on imminent herd immunity puts more pressure on Fauci and Biden to come clean… despite their variant-fearmongering and “no return to normal until Christmas or beyond” predictions.
But of course, this reality may never be allowed in the national narrative, as Makary previously concluded:
“Some medical experts privately agreed with my prediction that there may be very little Covid-19 by April but suggested that I not to talk publicly about herd immunity because people might become complacent and fail to take precautions or might decline the vaccine. But scientists shouldn’t try to manipulate the public by hiding the truth. As we encourage everyone to get a vaccine, we also need to reopen schools and society to limit the damage of closures and prolonged isolation. Contingency planning for an open economy by April can deliver hope to those in despair and to those who have made large personal sacrifices.“
But, but, the science!?
Coronavirus in the U.S.: Where cases are growing and declining – National Geographic
COVID-19 transmission continued to slow in the United States this week—although not as sharply as in recent weeks. New cases are down by 14 percent, while hospitalizations and deaths are down by 15.6 percent and 5 percent, respectively. A slower decline doesn’t necessarily mean the nation is approaching a plateau; the Presidents’ Day holiday and severe winter storms both interfered with case reporting across the country, according to the COVID Tracking Project. Also, the number of coronavirus infections remains relatively high, so people need to maintain protective measures, cautions White House advisor Anthony Fauci.
At the same time, concerns are rising that new coronavirus variants found in New York and California may be more contagious than the original virus. Cases attributed to the New York variant (B.1.526) have risen more than 12 percent in the last two weeks, while the California variant (B.1427/B.1429) makes up more than half of the cases in 44 counties across the state. The more contagious variant first spotted in the U.K. (B.1.1.7) has now been detected in 45 states, and the variants initially spotted in Brazil (P.1) and South Africa (B.1.351) have been identified in five and 15 states, respectively. To contain the spread, vaccination is all the more urgent. This week, Moderna announced that it has shipped doses of its booster vaccine for the South Africa variant to the National Institutes of Health for clinical study.

Op-Ed: With Variants, COVID-19 Race Becomes a Sprint – MedPage
We’re now in a race — a race for our lives as the COVID-19 virus continues to spread and escape our best defenses.
The latest competitors are variants of COVID-19, some of which are more transmissible and may cause more severe disease; and a public health community striving to get the virus under control by rapidly administering vaccines. Unfortunately, the vaccine rollout has been hamstrung by federal and state immunization campaigns that stumbled out of the gate.
In communities large and small, the playing field for vaccinating Americans is not level. People ages 65 and older living in multigenerational households can receive a vaccine in Washington state, for example, but that same group cannot get the vaccine a few miles away in Oregon.
Thankfully, we’ve gained critical ground over the past few weeks by getting millions of shots into arms while doubling down on mask wearing, hand-washing, and social distancing to prevent infection. Quickly vaccinating large numbers of people in the community reduces the opportunity for the virus to find new hosts.
At the finish line is herd immunity, the point at which most of a population is protected against an infectious disease, leaving the virus with nowhere else to go. Some have dubbed this “community immunity” because it calls upon each of us to do our part by getting vaccinated to keep our neighbors safe.
Winning the race against such an elusive opponent depends upon sufficient vaccine supply and effective distribution. The Biden administration is working to secure a total of 600 million doses to vaccinate 300 million Americans by the end of the summer or early fall.
We can meet this mark, but it will take our best efforts.
The emergence of COVID-19 variants in the U.K., Brazil, California, and South Africa add to the challenge. Some will be insignificant, while others like the one first found in South Africa and now detected in the U.S., may be more resistant to existing vaccines. This is where the race becomes a sprint, as researchers flex to develop booster shots to ward off the threat.
To further speed U.S. immunizations, an accelerated FDA approval process for new vaccines in the pipeline will help. Most importantly, coordinating a distribution network that moves vaccine from manufacturers to healthcare providers is critical. People want and should be able to get their shots from familiar trusted sources, wherever they may be.
A well-managed distribution network runs more like a relay race, requiring a smooth hand-off of the baton between all the key players — drug makers, the public health sector, pharmacies, health systems, and government officials. Federal agencies and vaccine manufacturers must collaborate to increase domestic production capacity, accelerate procurement and delivery of critical manufacturing equipment, and work with suppliers to increase production capacity for critical materials.
Community healthcare providers play an essential role in vaccinating people of color and disadvantaged populations. These populations are more likely to work in frontline industries, often live in overcrowded housing, and are less likely to have access to quality healthcare. Broad-based public-private partnerships to create mass vaccination sites will play a critical role in improving access to vaccines.
Frequently changing tiers and differing priorities at the federal, state, and local levels — which in effect forces players to switch lanes mid-race — has caused tremendous confusion, frustration, and dismay.
Open a window to reduce virus spread, CDC tells schools in new ventilation recommendations – CNN
The US Centers for Disease Control and Prevention posted new recommendations Friday on the importance of good ventilation in preventing coronavirus spread in schools and daycares. Its top recommendation: Open a window.
It’s the first time the agency has separately emphasized the role ventilation plays in helping or preventing the spread of the virus, which is transmitted in tiny particles called aerosols, as well as via larger articles.
“If safe to do so, open windows and doors,” the CDC advises. “Even just cracking open a window or door helps increase outdoor airflow, which helps reduce the potential concentration of virus particles in the air. If it gets too cold or hot, adjust the thermostat. Do not open windows or doors if doing so poses a safety or health risk (such as falling, exposure to extreme temperatures, or triggering asthma symptoms),” it adds.
“Open windows in transportation vehicles. Use exhaust fans in restrooms and kitchens.”
Mask use can prevent the virus from getting into the air in the first place, the CDC said on the newly posted web page. But good ventilation is also important.
“Use child-safe fans to increase the effectiveness of open windows. Safely secure fans in a window to blow potentially contaminated air out and pull new air in through other open windows and doors,” it adds. “Consider having activities, classes, or lunches outdoors when circumstances allow.”
The new guidance also addresses heating, ventilation and air conditioning (HVAC) systems. “Set HVAC systems to bring in as much outdoor air as your system will safely allow,” it suggests. “Increase the HVAC system’s total airflow supply to occupied spaces when you can. More air flow encourages air mixing and ensures any recirculated air passes through the filter more frequently.”
Filtration is also important, but filters should not reduce airflow.
The following are foreign headlines with hyperlinks to the posts
Ireland Sees Strong Early Evidence That Vaccines Are Working
Canada authorizes the AstraZeneca vaccine.
The following additional national and state headlines with hyperlinks to the posts
Want to Save Lives? Let Us Give COVID Vaccines in Our Offices, Docs Say
Real-World Data Tie COVID Vax to Drop in Intubation Rates
House Democrats pass sweeping $1.9T COVID-19 relief bill with minimum wage hike
FAA seeks to fine passenger accused of striking flight attendant $27,500
White House: COVID-19 Numbers Take a ‘Concerning Shift’
These Two Democrats Voted No on $1,400 Stimulus Checks
Storage Error Destroys Vaccine Doses for 1,000 Tennessee School District
Top health official in Memphis resigns after the state finds 2,400 wasted doses.
Supreme Court once again sides with houses of worship in dispute over Covid-19 restrictions
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
Future Output Loss From COVID-Induced School Closures
2021 Flu Report: Should Employers Embrace Post-Pandemic Mask-Wearing?
COVID-19 Across Counties With Different Pre-Pandemic Financial Distress
How Does The Johnson And Johnson Vaccine Compare To Other Coronavirus Vaccines? 4 Questions Answered
Warning to Readers
The amount of politically biased articles on the internet continues to increase. And studies and opinions of the experts continue to contradict other studies and expert opinions. Honestly, it is difficult to believe anything anymore.

I assemble this coronavirus update daily – sifting through the posts on the internet. I try to avoid politically slanted posts (mostly from CNN, New York Times, and the Washington Post) and can usually find unslanted posts on that subject from other sources on the internet. I wait to publish posts on subjects that I cannot validate across several sources. But after all this extra work, I do not know if I have conveyed the REAL facts. It is my job to provide information so that you have the facts necessary – and then it is up to readers to draw conclusions.
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19 when recovering from COVID-19. Herd immunity does not look like an option without immunization although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a significantly higher death rate as there is relatively few hospitalizations and deaths in younger age groups..
- There are at least 8 strains of the coronavirus. New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
What we do or do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work. Unfortunately, early in the pandemic, many health experts — in the U.S. and around the world — decided that the public could not be trusted to hear the truth about masks. Instead, the experts spread a misleading message, discouraging the use of masks.
- Current thinking is that we develop 5 months of immunity from further COVID infection.
- The Moderna and Pfizer vaccines have an effectiveness rate of about 95 percent after two doses. That is on par with the vaccines for chickenpox and measles. The 95 percent number understates the effectivenessas it counts anyone who came down with a mild case of Covid-19 as a failure. But turning Covid into a typical flu — as the vaccines evidently did for most of the remaining 5 percent — is actually a success. Of the 32,000 people who received the Moderna or Pfizer vaccine in a research trial, only one contracted a severe Covid case.
- To what degree do people who never develop symptoms contribute to transmission? Research early in the pandemic suggested that the rate of asymptomatic infections could be as high as 81%. But a meta-analysis, which included 13 studies involving 21,708 people, calculated the rate of asymptomatic presentation to be 17%.
- The accuracy of rapid testing is questioned – and the more accurate test results are not being given in a timely manner.
- Can children widely spread coronavirus? [current thinking is that they are a minor source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- Air conditioning contributes to the pandemic spread.
- It appears that there is increased risk of infection and mortality for those living in larger occupancy households.
- Male patients have almost three times the odds of requiring intensive treatment unit (ITU) admission compared to females.
- Outdoor activities seem to be a lower risk than indoor activities.
- Will other medical treatments for Covid-19 ease symptoms and reduce deaths? So far only remdesivir, Bamlanivimab,
and Regeneron) are approved for treatment. What drugs work?
Arthritis drugs tocilizumab and sarilumab could cut relative risk of death of those in intensive care by 24%
- A current scientific understanding of the way the coronavirus works can be found [here].
There is now a vaccine available – the questions remain:
- how effective it will be in the general population,
- will there be any permanent side effects that will appear months from now,
- how long immunity will last [we can currently say we do not know if it will last more than 4 months],
- there is no evidence the vaccine will block transmission
Heavy breakouts of coronavirus have hit farmworkers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>





