Written by Steven Hansen
The U.S. new cases 7-day rolling average are 15.5 % LOWER than the 7-day rolling average one week ago. U.S. hospitalizations due to COVID-19 are now 12.4 % LOWER than the rolling average one week ago. U.S. deaths due to coronavirus are now 6.4 % LOWER than the rolling average one week ago. Today’s posts include:
- U.S. Coronavirus New Cases are 121,469
- U.S. Coronavirus hospitalizations are at 91,440
- U.S. Coronavirus deaths are at 3,912
- U.S. Coronavirus immunizations have been administered to 10.1 % of the population
- The 7-day rolling average rate of growth of the pandemic shows new cases improved, hospitalizations improved, and deaths worsened
- Hopefully, these current improving COVID trends will remain in play even with the new strains
- Got a COVID vaccine? Here’s how to treat the side effects, including pain, swelling and more
- Using rapid tests in schools can cut coronavirus infection by half
- With a seductive number, AstraZeneca study fueled hopes that eclipsed its data
- The Mystery Of India’s Plummeting COVID-19 Cases
- International travel had ‘biggest impact’ in early COVID-19 spread
- Permanent damage and cardiovascular events following COVID-19 vaccination

The recent worsening of the trendlines for new cases is behind us which was attributed to going back to college/university, cooler weather causing more indoor activities, mutation of the virus, fatigue from wearing masks / social distancing, holiday activities, and some loosening of regulations designed to slow the coronavirus spread.
My continuing advice is to continue to wash your hands (especially after using the toilet as COVID first sheds in your stool), putting down the toilet seat (as flushing the toilet releases a plume), wear masks, avoid crowds, and maintain social distancing. No handwashing, mask, or social distancing will guarantee you do not get infected – but it sure as hell lowers the risk in all situations – and the evidence to-date shows a lower severity of COVID-19. In addition, certain activities are believed to carry a higher risk – like being inside in air conditioning and removing your mask (such as restaurants, around your children/grandchildren, bars, and gyms). It is all about viral load – and outdoor activities are generally safe if you can maintain social distance. Finally, studies show eating right (making sure you are supporting your immune system) and adequate sleep increase your ability to fight off COVID.
include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus1.htm’); ?>
Hospitalizations (grey line) and Mortality (green line)
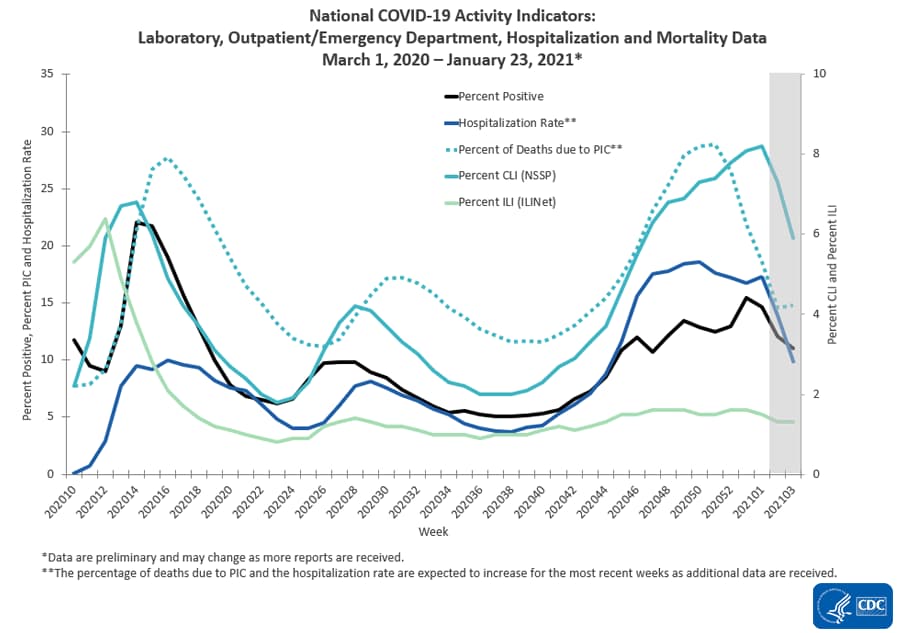
source: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html
Hospitalizations Are The Only Accurate Gauge As Reporting Is Not Affected By Holidays
The 4 day Thanksgiving holiday period put the first wobble in the trends. Over weekends and holidays, the number of new cases and deaths decline. Over weekends, this is not a problem for week-over-week rolling averages as weekends are compared against the previous weekend. But when a holiday falls within a working week, a non-working day is compared to a working day which causes havok in the trends.
However, hospitalizations historically appear to be little affected by weekends or holidays – the daily counts do not vary significantly from day-to-day.
The hospitalization growth rate trend is improving.

For the Thanksgiving and the end of the year holiday period – roughly, it seems each appears to have added around 5 % to the rate of growth of new cases, hospitalizations, and deaths.
Historically, hospitalization growth follows new case growth by one to two weeks.
As an analyst, I use the rate of growth to determine the trend. But, the size of the pandemic is growing in terms of real numbers – and if the rate of growth does not become negative – the pandemic will overwhelm all resources.
The graph below shows the rate of growth relative to the growth a week earlier updated through today [note that negative numbers mean the rolling averages are LOWER than the rolling averages one week ago]. As one can see, the rate of growth for new cases peaked in early December 2020 for Thanksgiving, and early January 2021 for end of year holidays – and the rate of growth is now contracting.

In the scheme of things, new cases decline first, followed by hospitalizations, and then deaths.
It is up to each of our readers to protect themselves and others by washing your hands, wearing a mask, avoiding crowds, and maintaining social distancing.
Will The New Variants Cause The Next Spike?
Maybe and maybe not. It all depends on vaccinations:
- the more people that are vaccinated reduces the pool of people that can be infected. Today we have removed over 10 % of the population from being infected which theoretically should reduce the infection rate by 10 % [it is unstudied whether the vaccines prevent a vaccinated person from being a carrier of the virus even though showing no signs]. If the vaccines are shown to stop transmission, then in theory it would reduce the infection rate by double the percent vaccinated [in this case you prevent your own infection and do not pass it along to another].
- it is also unknown what the effective rate of the current vaccines is against mutations that seem to appear almost daily. As an example, if the effective rate drops to 60%, it means the 10 % reduction in the infection rate discussed above is almost cut in half. The South African and Brazilian variant is somewhat immune to the current vaccines.
- The pandemic should be over immediately if everyone could be vaccinated today. The problem is that every day brings a new mutation (which would not appear if the pandemic was stopped). The longer the immunization process takes – the more ineffective the vaccine will become.
- It is not clear whether the vaccine prevents those vaccinated from spreading the virus. It seems to be well documented that it normally stops the virus from taking hold and when it does not – the infection is mild.
Coronavirus News You May Have Missed
Using rapid tests in schools can cut coronavirus infection by half, study finds – CNN
Weekly screening of all students, teachers, and staff using rapid antigen tests can reduce in-school infections by 50% for high schools and 35% for primary schools, a new study found.
The different results between high schools and primary schools are due to high schoolers having a greater number of contacts and higher rates of transmission, according to the study by the Rockefeller Foundation and the Department of Health and Human Services
How the study was conducted: From October to December 2020, 20,000 rapid antigen tests were distributed to K-12 schools in six pilot cities across the United States.
Each city used these tests to develop independent school testing programs aligned with guidelines developed by Johns Hopkins University and Duke-Margolis Center for Health Policy.
Schools had to decide how often to test, if testing should take place on or off school grounds and how to approach staff and students opting out of testing.
Other findings: The analysis also found that monthly testing showed a 5% reduction in infections, while twice weekly testing showed a 20% reduction. It also found that testing only teachers and staff is less effective, and the impact is greater in high schools, where students typically attend multiple classes in a day.
Social distancing by 6 feet or more can reduce infections by 88%, and universal masking by 40%, the study said.
The Mystery Of India’s Plummeting COVID-19 Cases – NPR
Last September, India was confirming nearly 100,000 new coronavirus cases a day. It was on track to overtake the United States to become the country with the highest reported COVID-19 caseload in the world. Hospitals were full. The Indian economy nosedived into an unprecedented recession.
But four months later, India’s coronavirus numbers have plummeted. Late last month, on Jan. 26, the country’s Health Ministry confirmed a record low of about 9,100 new daily cases — in a country of nearly 1.4 billion people. It was India’s lowest daily tally in eight months. On Monday, India confirmed about 11,000 cases.
“It’s not that India is testing less or things are going underreported,” says Jishnu Das, a health economist at Georgetown University. “It’s been rising, rising — and now suddenly, it’s vanished! I mean, hospital ICU utilization has gone down. Every indicator says the numbers are down.”
Scientists say it’s a mystery. They’re probing why India’s coronavirus numbers have declined so dramatically — and so suddenly, in September and October, months before any vaccinations began.
Mask and mandates
India is one of several countries — mostly in Asia, Africa and South America — that have mandated masks in public spaces. Prime Minister Narendra Modi appeared on TV wearing a mask very early in the coronavirus pandemic. The messaging was clear.
In many Indian municipalities, including the megacity Mumbai, police hand out tickets — fines of 200 rupees ($2.75) — to violators. Mumbai’s mask mandate even applies outdoors, to joggers on the beach and passengers in open-air rickshaws.
Heat and humidity
Aside from mask compliance, there’s also India’s climate: Most of the country is hot and humid. That too has deepened the mystery. There’s some evidence that India’s climate may help reduce the spread of respiratory viruses. But there’s also some evidence to the contrary.
A review of hundreds of scientific articles, published in September in the journal PLOS One, found that warm and wet climates seem to reduce the spread of COVID-19. Heat and humidity combine to render coronaviruses less active — though the certainty of that conclusion, the review says, is low. Previous research has also found that droplets of the virus may stay afloat longer in air that’s cold and dry.
“When the air is humid and warm, [the droplets] fall to the ground more quickly, and it makes transmission harder,” Elizabeth McGraw, director of the Center for Infectious Disease Dynamics at Pennsylvania State University, told NPR last year. (However, the science of transmission is still evolving.)
Prevalence of other diseases
Another point to consider about India is how many other diseases are already rampant: malaria, dengue fever, typhoid, hepatitis, cholera. Millions of Indians also lack access to clean drinking water, sanitation and hygienic food. Some experts speculate that people with robust immune systems may be more likely to survive in India in the first place.
“All of us have pretty good immunity! Look at the average Indian: He or she has probably had malaria at some point in his life or typhoid or dengue,” says Sayli Udas-Mankikar, an urban policy expert at the Observer Research Foundation in Mumbai. “You end up with basic immunity toward grave diseases.”
Demographics
India is a very young country as well. Only 6% of Indians are older than 65. More than half the population is under 25. Those who are young are less likely to die of COVID-19 and are more likely to show no symptoms if infected.
A study of nearly 85,000 coronavirus cases in India, published in November in the journal Science, found that the COVID-19 mortality rate actually decreases there after age 65 — possibly because Indians who live past that age are such outliers. There are so few of them.
Timing
India’s climate and demographics have not changed during the pandemic. And the drop in India’s COVID-19 caseload has been recent. It hit a peak in September and has declined inexplicably since then.
In fact, India’s numbers went down exactly when experts predicted they would spike: in October, when millions of people gathered for the Hindu festivals of Diwali and Durga Puja. It’s when air pollution is also worst, and experts feared that would exacerbate the pandemic too.
Cases have also declined despite what many thought would be a superspreader event: tens of thousands of Indian farmers camping out on the capital’s outskirts for months.
Permanent damage and cardiovascular events following COVID-19 vaccination – Final Warning
More doctors are speaking out about the harms of new COVID-19 vaccines. Cardiothoracic surgeon, Dr. Hooman Noorchashm, M.D., Ph.D. is one of them. Dr. Noorchashm says that the covid-19 vaccines will almost certainly cause an antigen-specific immune response; however, if viral antigens are present in the tissues of recipients at the time of vaccination, the vaccine-augmented immune response will turn the immune system against those tissues, causing inflammation that can lead to blood clot formation. This destructive auto-immune effect could do significant damage to endothelial cells of elderly patients who already suffer from cardiovascular disease. There have already been numerous reports of unexplained cardiovascular fatalities following covid-19 vaccination across Norway, Germany, the UK, Gibraltar and the United States.
Dr. Noorchashm’s findings are consistent with the research findings of Dr. J. Patrick Whelan, M.D., Ph.D., who shared similar concerns with the FDA in early December of 2020. Whelan warned that a recently-infected patient who is subject to covid-19 vaccination is likely to suffer from autoimmune attacks along the ACE-2 receptors present in the heart, and in the microvasculature of the brain, liver and kidney. The risk is doubled because two shots are required. It is a well documented fact that SARS-CoV-2, the Wuhan coronavirus, readily targets humans through the vascular endothelium. The virus is known to enter into endothelial cells through the ACE-2 receptor on the endothelium. Because of this unique gain-of-function, one of the medical emergencies that may occur in covid-19 patients is thromboembolic complications (formation of a blood clot inside a blood vessel). If viral antigens are present in the endothelial lining of blood vessels, then the vaccine will cause an antigen-specific immune response that attacks those precious tissues, potentially causing cardiovascular events.
With a seductive number, AstraZeneca study fueled hopes that eclipsed its data – STAT
A new paper released this week suggested that a vaccine developed by AstraZeneca and Oxford University not only protected clinical trial participants from developing disease, but also may significantly reduce transmission of the virus that causes the disease.
In the recent burst of data on Covid-19 vaccines, that suggestion stood out. The question of whether Covid-19 vaccines reduce transmission has been a critical and unanswered one, creating uncertainty over whether people who have been vaccinated will still be able to be infected by and transmit onward SARS-Cov-2, the virus that causes Covid, to those who have not yet been vaccinated.
Media reports seized on a reference in the paper from Oxford researchers that a single dose of the vaccine cut positive test results by 67%, pointing to it as the first evidence that a vaccine could prevent transmission of the virus. But the paper, which has not yet been peer-reviewed, does not prove or even claim that — although it hints at the possibility.
Instead, it showed that fewer people were carrying the virus as a result of being vaccinated. Fewer people carrying virus, the researchers argued, would equate to a reduction in the amount of virus circulating in a community.
“These data indicate that [the AstraZeneca vaccine], used in the authorised schedules, may have a substantial impact on transmission by reducing the number of infected individuals in the population,” the authors wrote.
If a person tests negative, Andrew Pollard, one of the study authors and a professor of pediatric infection and immunity at the University of Oxford, told STAT via email, “then it is a reasonable assumption that they cannot transmit.”
But it is a big and unjustified leap, outside experts agree, from that suggestion to proof of decreased transmission from people who are vaccinated.
“The study showed a decrease in [viral] shedding, not ‘transmission,'” said Carlos del Rio, a professor of infectious diseases at the Emory University School of Medicine. “The bottom line is, no, one cannot draw a conclusion or straight line.”
Kathleen Neuzil, director of the Center for Vaccine Development at the University of Maryland School of Medicine, concurred.
“There are too many, in my view, moving variables to make too much of one single result here,” she said. “The trend, though, is consistent and in the right direction.”
Got a COVID vaccine? Here’s how to treat the side effects, including pain, swelling and more – USA Today
How to treat COVID-19 vaccine injection site pain:
One area that may react to the vaccine is the arm where you received the shot. The Centers for Disease Control and Prevention lists injection site pain and swelling as normal side effects. Here are some things you can do:
Pain relievers: Though the CDC and the World Health Organization recommend against the preventive use of over-the-counter pain relief medications such as acetaminophen or ibuprofen, they do allow them if symptoms develop after the shot. Daignault recommends checking with your doctor first, however, if you’re already taking other medications.
Cool it down: “Ice is a great treatment for swelling – plus for pain, and it’s often overlooked but it’s something we all have and it doesn’t interact with any medications you have already,” Daignault said. Out of ice? The CDC says you can use a “clean, cool, wet washcloth over the area” as well.
Epsom salt baths: “If it’s really sore or if you have general body aches,” Daignault said, “just take 2 cups of Epsom salt, put it in some relatively warm water and soak in there for 20 minutes, finish with a cold shower and get into bed.”
Exercise your arm: “The muscle ache comes from localized inflammation,” Dr. Richard Pan, a pediatrician and California State Senator who chairs the Senate Committee on Health, explained to USA TODAY. “So moving the arm around can sometimes make it feel better.”
How to treat general COVID-19 vaccine symptoms:
You may also experience symptoms including fever, chills, tiredness and headaches.
Rest up: “I would say rest as much as you can,” Daignault said, before advising not to over-do it. “I’m also encouraging people to go about their daily activities… because you always want to maintain the best cardiovascular system as possible.”
Drink fluids: The CDC recommends this as a way to “reduce discomfort from fever.”
Dress lightly: The CDC also recommends this for fevers.
International travel had ‘biggest impact’ in early COVID-19 spread – The Hill
The biggest factor in the death rate from the first wave of coronavirus cases was international travel, according to a new study from researchers at the University of Aberdeen.
Researchers assessed death rates in the 37 hardest-hit countries, looking at factors including urban population, population density and arrivals at the border. Countries analyzed included the U.S., the United Kingdom, Spain, France, Italy and Brazil.
According to the research, published in BMJ Open, every 1 million international arrivals was associated with a 3.4 percent spike in the mean daily increase of deaths from the virus.
“Our assessment of available data indicates that very early restrictions on international travel might have made a difference in the spread of pandemic in western Europe, including the UK,” co-author Tiberiu Pana said in a statement. “These findings are particularly important as the world looks to control future waves and strains of the COVID-19 pandemic and prevent related deaths.”
The data also indicate a country’s rates pf Bacillus Calmette-Guérin vaccination may also be associated with a reduction in death rates, Tiberiu said.
“Nevertheless, these associations were weaker and further work looking at individual patients is required to clarify these potential relationships,” he added.
Travelers may soon need proof of a Covid-19 vaccination or a negative virus test. – New York Times
Among governments and those in the travel industry, a new term has entered the vocabulary: vaccine passport.
One of President Biden’s executive orders asks government agencies to “assess the feasibility” of linking coronavirus vaccine certificates with other vaccination documents, and producing digital versions of them.
The Danish government said on Wednesday that it would introduce a “digital passport” in the next few months that can be used as proof of vaccination.
In a few weeks, two airlines, Etihad Airways and Emirates, will start using a digital travel pass, developed by the International Air Transport Association, that, among other things, provides airlines and governments with documentation that passengers have been vaccinated or tested for the coronavirus.
The challenge is creating a universal document or app that protects privacy and is accessible regardless of people’s wealth or access to smartphones.
“It’s about trying to digitize a process that happens now and make it into something that allows for more harmony and ease, making it easier for people to travel between countries without having to pull out different papers for different countries,” said Nick Careen, senior vice president for airport, passenger, cargo and security at I.A.T.A., where he has been leading the travel pass initiative.
Covid-19 variants from South Africa and Brazil are hard to detect in the US, expert says – CNN
The United States has identified hundreds of cases of a more contagious strain first linked to the UK — but two others, linked to South Africa and Brazil, are much harder to find, according to Dr. James Lu, president of a company called Helix, whose Covid-19 tests have helped identify many of these cases.
It’s the latter two strains that may be more concerning when it comes to vaccine efficacy and reinfection, experts say.
Part of the reason why we’ve found so many cases of B.1.1.7 — the strain first detected in the UK — is because of a testing glitch that picks up one if its mutations.
Not all samples with this glitch are the B.1.1.7 strain, since this mutation can exist on its own. And not all brands of PCR tests show this glitch, called S gene dropout. But it has been used to screen for potential cases of the variant, which must then be confirmed through genetic sequencing.
“S gene dropout gives us a really good way to enrich for the samples of B.1.1.7,” Lu told CNN. “That said, if you were just sampling randomly across the country, it’s much harder to detect.”
The mutation that causes this glitch is not present in the strains first spotted in South Africa and Brazil.
Beyond appearing more transmissible, these two strains also contain a different mutation that scientists worry could help the virus escape some of the antibody protection from vaccines or previous infection. Even so, experts say they expect vaccines will still work against the variants — especially when it comes to preventing severe disease and death.
“They’re not detectable with our level of sampling today,” Lu said of variants linked to South Africa and Brazil. “So, most of the time, if we’re finding it, it’s serendipity right now. But that will change if they become more prevalent.”
The following are foreign headlines with hyperlinks to the posts
WHO: Decline in Global Coronavirus Cases Shows Variants Can Be Controlled
Czech 1M: The Czech Republic has reached 1 million confirmed cases. It is by far the smallest of the 21 countries to surpass the milestone, with the U.S. leading the global table with more than 26 million
France ICU: The ICU ward at the biggest hospital in southern France is facing a constant, steady flow of virus patients.
Gulf Arab states are launching new restrictions over fears of the coronavirus resurging across their countries.
One of the World Health Organization investigators looking for clues into the origin of the coronavirus in the central Chinese city of Wuhan says the Chinese side has provided a high level of cooperation.
Hong Kong continues to force “ambush-style” lockdowns of entire residential blocks as part of its strategy to contain the virus. (The Guardian)
Australian Open Players Quarantining After Tournament Worker Tests Positive For Virus
WHO Team Probing COVID-19 Visits Wuhan Lab, Meets ‘Bat Woman’
Red Cross warns of ‘devastating’ consequences as poorer countries struggle to secure vaccines.
Early-stage trials for a Chinese vaccine show encouraging results in older adults
A trial is being launched in the U.K. to explore whether using different Covid-19 vaccines for the first and second doses works, in a bid to make nationwide vaccination programs more flexible.
Cuba will implement a nightly curfew in Havana to combat Covid-19 spread
Denmark plans to introduce a digital “vaccine passport” in an effort to reopen society, help businesses and ease travel, the government announced Wednesday. The scheme would initially apply to business travelers but authorities hope it could also help the country reopen, allowing Danes to go to restaurants, conferences, music festivals and sporting events — all of which have been restricted since a nationwide lockdown was imposed in December.
All Israelis from 16 years up now eligible for Covid-19 vaccination
The following additional national and state headlines with hyperlinks to the posts
American Airlines warns 13000 employees of potential furloughs
U.S. COVID cases continue to fall, even with one-day death rate still above 3,000
AP investigation of Catholic Church and US aid. An AP investigation has found that scores of Roman Catholic dioceses in the U.S. had more than $10 billion in cash and other readily available funds when they received at least $1.5 billion from the federal government’s small business emergency relief program.
Vaccine-Virus Transmission: A new study may help answer answer one of the major questions about the campaign to suppress the outbreak. Researchers from Oxford University say AstraZeneca’s vaccine does more than protect people from falling seriously ill — it also has the potential to reduce transmission of the virus.
Whichever team you’re rooting for and whichever commercial is your favorite, please watch the Super Bowl safely, gathering only virtually or with the people you live with,” said CDC Director Rochelle Walensky, MD, MPH.
The University of California Davis is now offering free coronavirus tests, masks, and quarantine housing for all local residents and workers, university-affiliated or not.
Daily COVID tests have stagnated in the U.S. since a high of 2 million in mid-January, and this is a problem.
SARS-CoV-2 can infect human pancreatic tissue and result in metabolic dysregulation, according to a paper in Nature Metabolism.
Inhaled aviptadil (Zyesami) moves onto phase II/III clinical study in early-stage COVID, NeuroRx announced.
HHS gives cold shoulder to victims of vaccine injury
The number of Americans seeking unemployment benefits declined to 779,000 last week.
One-third say financial struggles made them relocate during pandemic
US Community Health Centers Say They Have Given More Vaccines Than Government Data Show
Who Could Receive a Third Stimulus Check? Debate Could Lower Eligibility – President Joe Biden won’t negotiate on the $1,400 payment amount, but said he’s open to reducing the number of people who are eligible.
Man Stole Vehicle Containing COVID Vaccine Doses, Florida Police Say
Shocking video shows maskless market in Naples, Florida
Kansas Reports Case of U.K. COVID Variant That May Be More Deadly – CDC director Rochelle Walensky said “increasing data” suggests B.1.1.7 may cause more deaths than past forms of the virus.
Black Americans are sharply divided by age and gender over Covid vaccines.
All Capitol Police officers will be vaccinated, the acting chief says.
California-based drone delivery start-up Zipline is developing cold-chain storage, and starting this April, it plans to have drones that can deliver frozen and ultra-low temperature Covid-19 vaccines and medical products in the markets where it operates
Supermarket workers angry as Kroger plans store closures to avoid pandemic hazard payments
LGBTQ community may be more vulnerable to Covid-19, CDC says
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
December 2020 Headline Manufacturing New Orders Improvement Continued
30 January 2021 New York Fed Weekly Economic Index (WEI): Index Decline Continues
4Q2020 Preliminary Headline Productivity Contracts
30 January 2021 Initial Unemployment Claims Rolling Average Marginally Improves
January 2021 Job Cuts Increase Slightly
Warning to Readers
The amount of politically biased articles on the internet continues to increase. And studies and opinions of the experts continue to contradict other studies and expert opinions. Honestly, it is difficult to believe anything anymore. A study usually cannot establish cause and effect – but only correlation. Be very careful what you believe about this pandemic.

I assemble this coronavirus update daily – sifting through the posts on the internet. I try to avoid politically slanted posts (mostly from CNN, New York Times, and the Washington Post) and can usually find unslanted posts on that subject from other sources on the internet. I wait to publish posts on subjects that I cannot validate across several sources. But after all this extra work, I do not know if I have conveyed the REAL facts. It is my job to provide information so that you have the facts necessary – and then it is up to readers to draw conclusions.
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19 when recovering from COVID-19. Herd immunity does not look like an option without immunization although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a significantly higher death rate as there is relatively few hospitalizations and deaths in younger age groups..
- There are at least 8 strains of the coronavirus. New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
What we do or do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work. Unfortunately, early in the pandemic, many health experts — in the U.S. and around the world — decided that the public could not be trusted to hear the truth about masks. Instead, the experts spread a misleading message, discouraging the use of masks.
- Current thinking is that we develop 5 months of immunity from further COVID infection.
- The Moderna and Pfizer vaccines have an effectiveness rate of about 95 percent after two doses. That is on par with the vaccines for chickenpox and measles. The 95 percent number understates the effectivenessas it counts anyone who came down with a mild case of Covid-19 as a failure. But turning Covid into a typical flu — as the vaccines evidently did for most of the remaining 5 percent — is actually a success. Of the 32,000 people who received the Moderna or Pfizer vaccine in a research trial, only one contracted a severe Covid case.
- To what degree do people who never develop symptoms contribute to transmission? Research early in the pandemic suggested that the rate of asymptomatic infections could be as high as 81%. But a meta-analysis, which included 13 studies involving 21,708 people, calculated the rate of asymptomatic presentation to be 17%.
- The accuracy of rapid testing is questioned – and the more accurate test results are not being given in a timely manner.
- Can children widely spread coronavirus? [current thinking is that they are a minor source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- Air conditioning contributes to the pandemic spread.
- It appears that there is increased risk of infection and mortality for those living in larger occupancy households.
- Male patients have almost three times the odds of requiring intensive treatment unit (ITU) admission compared to females.
- Outdoor activities seem to be a lower risk than indoor activities.
- Will other medical treatments for Covid-19 ease symptoms and reduce deaths? So far only remdesivir, Bamlanivimab,
and Regeneron) are approved for treatment. What drugs work?
Arthritis drugs tocilizumab and sarilumab could cut relative risk of death of those in intensive care by 24%
- A current scientific understanding of the way the coronavirus works can be found [here].
There is now a vaccine available – the questions remain:
- how effective it will be in the general population,
- will there be any permanent side effects that will appear months from now,
- how long immunity will last [we can currently say we do not know if it will last more than 4 months],
- there is no evidence the vaccine will block transmission
Heavy breakouts of coronavirus have hit farmworkers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>





