Written by Steven Hansen
The U.S. new cases 7-day rolling average is 27.0 % HIGHER than the 7-day rolling average one week ago. U.S. hospitalizations due to COVID-19 are now 4.8 % HIGHER than the rolling average one week ago. U.S. deaths due to coronavirus are now 19.1 % HIGHER than the rolling average one week ago. Today’s posts include:
- U.S. Coronavirus New Cases are at an elevated 283,,204
- U.S. Coronavirus hospitalizations are at an elevated 131,889
- U.S. Coronavirus deaths are at an elevated 3,456
- U.S. Coronavirus immunizations have been administered to 2.0 % of the population
- The 7-day rolling average rate of growth of the pandemic shows new cases worsened, hospitalizations worsened, and deaths worsened
- Moderna says second dose of its Covid-19 can be effectively administered up to 42 days after first dose
- Physician Assistant Who Sounded COVID Alarm Had Long Recovery
- Pfizer says its vaccine works against one of the key mutations in the variants found in Britain and South Africa
- Experts torn over changing vaccine doses to speed up lagging rollout
- What the data show about allergic reactions to COVID-19 vaccines
- Nanoparticle vaccine for COVID-19
- Study Confirms Key COVID-19 Risk Factors in Children
- No Need to Stop RAS Inhibitors in COVID-19

The recent worsening of the trendlines for new cases should be attributed to going back to college/university, cooler weather causing more indoor activities, possible mutation of the virus, fatigue from wearing masks / social distancing, holiday activities, political rallies / voting, and continued loosening of regulations designed to slow the coronavirus spread.
My continuing advice is to continue to wash your hands (especially after using the toilet as COVID first sheds in your stool), putting down the toilet seat (as flushing the toilet releases a plume), wear masks, avoid crowds, and maintain social distancing. No handwashing, mask, or social distancing will guarantee you do not get infected – but it sure as hell lowers the risk in all situations – and the evidence to-date shows a lower severity of COVID-19. In addition, certain activities are believed to carry higher risk – like being inside in air conditioning and removing your mask (such as restaurants, around your children/grandchildren, bars, and gyms). It is all about viral load – and outdoor activities are generally safe if you can maintain social distance. Finally, studies show eating right (making sure you are supporting your immune system) and adequate sleep increase your ability to fight off COVID.
include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus1.htm’); ?>
Hospitalizations (grey line) and Mortality (green line)
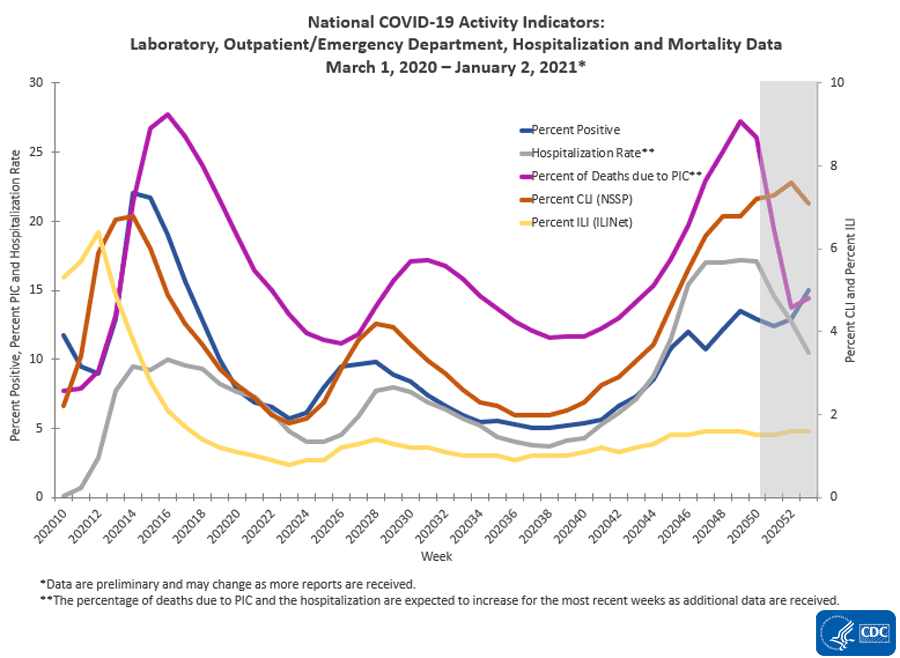
source: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html
The Impact of Holidays – Hospitalizations Are The Only Accurate Gauge As Reporting Is Sporadic
The 4 day Thanksgiving holiday period put a wobble in the trends. Over weekends and holidays, the number of new cases and deaths decline. Over weekends, this is not a problem for week-over-week rolling averages as weekends are compared against the previous weekend. But when a holiday falls within a working week, a non-working day is compared to a working day which causes havok in the trends. Now we are faced with the end of the year holiday season which means reporting is sporadic and numbers will initially look good – and then as the holidays end and the reporting catches up, the numbers will look terrible. In addition, family gatherings and travel will cause more virus transmission.
However, hospitalizations historically appear to be little affected by weekends or holidays – the daily counts do not vary significantly from day-to-day.
The hospitalization growth rate trend is growing at an ever slowing growth rate which is all good news as it means the number of beds needed is currently growing around 4 % every week.

For the Thanksgiving holiday period – roughly, it seems to have added around 5 % to the rate of growth of new cases, hospitalizations, and deaths.
Historically, hospitalization growth follows new case growth by one to two weeks.
As an analyst, I use the rate of growth to determine the trend. But, the size of the pandemic is growing in terms of real numbers – and if the rate of growth does not become negative – the pandemic will overwhelm all resources.
The graph below shows the rate of growth relative to the growth a week earlier updated through today [note that negative numbers mean the rolling averages are LOWER than the rolling averages one week ago]. As one can see, the rate of growth for new cases peaked in early December 2020 ago and the rate of growth has been decelerating since.

In the scheme of things, new cases decline first, followed by hospitalizations, and then deaths.
It is up to each of our readers to protect themselves and others by washing your hands, wearing a mask, avoiding crowds, and maintaining social distancing.
We Are Likely In A Pandemic Surge Caused By The Holidays And Virus Mutation
The “experts” will tell you they told you so – and you should have stayed at home instead of traveling to be with the people you care about. And there is some truth in this opinion.
But there will be no way to accurately understand the impact of the holidays because there are new mutant strains of the coronavirus that are more transmissible.
To gauge the impact of anything, you change ONLY ONE variable at a time (and hopefully in a controlled environment). There are now two variables in play – and it is nearly impossible to separate the impact of each.
Coronavirus News You May Have Missed
Physician Assistant Who Sounded COVID Alarm Had Long Recovery – MedPage
James Cai, the physician assistant who was New Jersey’s first COVID-19 patient, no longer needs supplemental oxygen and has been back to work for several months, seeing a steady drumbeat of coronavirus patients.
Back in March, Cai made headlines for warning the country that even young, relatively healthy 32-year-olds like himself were vulnerable to the virus, which was still largely a mystery in the U.S. at the time. He was worried that he wasn’t getting the right treatment at the hospital, so he took his case to Twitter.
“In the beginning, they just treat me like normal flu. They say I’m young, I’m not going to die, but they don’t know the truth about corona[virus],” Cai said during an interview posted to Twitter at the time. That interview was with Bill Pulte, a self-described Twitter philanthropist and grandson of home-construction magnate William Pulte, and it propelled him into the national spotlight — including a profile in the New York Times in April.
Cai was admitted to the hospital on March 3. He received high-flow oxygen, chloroquine, and lopinavir/ritonavir (Kaletra), and was one of the first patients to receive remdesivir under compassionate use. He worked his connections to reach out to Chinese physicians who’d treated the disease, and a Chinese-American doctor translated Chinese protocols into English for Cai’s New Jersey doctors.
He was discharged on March 21, needing supplemental oxygen — especially at night.
Cai didn’t respond to MedPage Today‘s requests for an interview, but his Twitter feed has provided significant insights into his recovery.
Within a month of his discharge, on April 20, he went back to work as a physician assistant, but only virtually. Two months after that, as coronavirus cases began to ease in New Jersey, he went back to practicing in the clinic.
But even in mid-summer, Cai was still seeing impairments in his oxygen saturation and activity levels.
“My O2 is 97% when I am awake but it does drop to 90% when I lay down for few hours or fall into sleep,” he tweeted on July 18. “I still need O2 to sleep & do get tired very easily. I used to work 60-70 hours a week by working in the clinic, nursing home, outpatient surgery, and play[ing] with my daughter at home. Now I only work 30 hrs in the clinic. … Plus I couldn’t run and exercise like before,” he said in another tweet that day.
[editor’s note: there is interesting information in the article, and worth a full read]
Experts torn over changing vaccine doses to speed up lagging rollout – National Geographic
AS COVID-19 CASES surge across the U.S., officials are facing increasing pressure to dole out vaccine doses as quickly as possible.
Today, a spokesperson for the transition team of President-elect Joseph R. Biden, Jr. said the new administration plans to release additional doses of the vaccine to prioritize getting people their first shots. The announcement comes amid proposals that would alter the ways the vaccines are administered to meet the urgent crisis—even if that goes against the proven regimens from vaccine makers and the recommendations of leading experts on infectious disease.
As of publication, about 21 million doses of the two vaccines authorized for use in the U.S. have been distributed across the country—but fewer than six million have been given to patients. Most experts interviewed for this article agreed the U.S. is not facing a vaccine shortage. Instead, the nation is grappling with a combination of a slower-than-anticipated rollout, rising COVID-19 cases, and the arrival of a new, more transmissible variant of the virus.
Earlier this week, Operation Warp Speed Chief Advisor Moncef Slaoui raised the possibility of halving the doses of the vaccine created by biotechnology company Moderna. In response, the National Institutes of Health announced it would work with Moderna to examine the efficacy of administering lower doses of the vaccine, which showed 95-percent efficacy in trials of its full dosage. In theory, this tactic would double the amount of the vaccine available in the country while still allowing people who get vaccinated to receive two shots.
Tinkering with the dosage rather than developing more effective ways to use existing stock is “the right answer to the wrong question,” says Anthony Fauci, the longtime director of the National Institute of Allergy and Infectious Diseases. “The disconnect is not that we want to stretch out the doses, but we want to be more efficient in getting the vaccine into people. If the time comes that we don’t have enough vaccine, then you should seriously consider the half-dose approach.”
… One issue in considering the reduced dosage is that an immune response is not the same thing as proven protection against a disease, warns Paul Offit, director of the Vaccine Education Center at the Children’s Hospital of Philadelphia and a government adviser on vaccine policy. While the presence of antibodies often means that a patient has developed some immune protection, it’s not a given. For example, people can have antibodies against HIV without being protected from the disease. To say that immune response means protection, Offit says, “is to ignore history.”
… it makes sense, in the context of the crisis, to “give more people the first dose” even if that means delaying a second shot. “Even though we’ve got inadequate data to be entirely sure about what we’re doing here, there is enough data to make a necessarily rapid judgment under the circumstances that will save lives, and will take pressure off our healthcare service,” he says.
[editor’s note: interesting debate – article deserves a full read]
Nanoparticle vaccine for COVID-19 – Science Daily
Before the pandemic, the lab of Stanford University biochemist Peter S. Kim focused on developing vaccines for HIV, Ebola and pandemic influenza. But, within days of closing their campus lab space as part of COVID-19 precautions, they turned their attention to a vaccine for SARS-CoV-2, the virus that causes COVID-19. Although the coronavirus was outside the lab’s specific area of expertise, they and their collaborators have managed to construct and test a promising vaccine candidate.
“Our goal is to make a single-shot vaccine that does not require a cold-chain for storage or transport. If we’re successful at doing it well, it should be cheap too,” said Kim, who is the Virginia and D. K. Ludwig Professor of Biochemistry. “The target population for our vaccine is low- and middle-income countries.”
Their vaccine, detailed in a paper published Jan. 5 in ACS Central Science, contains nanoparticles studded with the same proteins that comprise the virus’s distinctive surface spikes. In addition to being the reason why these are called coronaviruses — corona is Latin for “crown” — these spikes facilitate infection by fusing to a host cell and creating a passageway for the viral genome to enter and hijack the cell’s machinery to produce more viruses. The spikes can also be used as antigens, which means their presence in the body is what can trigger an immune response.
Nanoparticle vaccines balance the effectiveness of viral-based vaccines with the safety and ease-of-production of subunit vaccines. Vaccines that use viruses to deliver the antigen are often more effective than vaccines that contain only isolated parts of a virus. However, they can take longer to produce, need to be refrigerated and are more likely to cause side effects. Nucleic acid vaccines — like the Pfizer and Moderna mRNA vaccines that have recently been authorized for emergency use by the FDA — are even faster to produce than nanoparticle vaccines but they are expensive to manufacture and may require multiple doses. Initial tests in mice suggest that the Stanford nanoparticle vaccine could produce COVID-19 immunity after just one dose.
The researchers are also hopeful that it could be stored at room temperature and are investigating whether it could be shipped and stored in a freeze-dried, powder form. By comparison, the vaccines that are farthest along in development in the United States all need to be stored at cold temperatures, ranging from approximately 8 to -70 degrees Celsius (46 to -94 degrees Fahrenheit).
Study Confirms Key COVID-19 Risk Factors in Children – Medscape
Children and adolescents who receive positive COVID-19 test results are not only more likely to have been in close contact with someone with a confirmed case of the virus but also are less likely to have reported consistent mask use among students and staff inside the school they attended, reported Charlotte V. Hobbs, MD, and colleagues at the University of Mississippi, Jackson.
n partnership with the Centers for Disease Control and Prevention’s COVID-19 Response Team, Hobbs and colleagues conducted a case-control study of 397 children and adolescents under 18 years of age to assess school, community, and close contact exposures associated with pediatric COVID-19. Patients tested for COVID-19 at outpatient health centers or emergency departments affiliated with the University of Mississippi Medical Center between Sept. 1 and Nov. 5, 2020, were included in the study.
Nearly Two-Thirds Reported That Exposure Came From Family Members
Of the total study participants observed, 82 (21%) were under 4 years of age; 214 (54%) were female; 217 (55%) were non-Hispanic black, and 145 (37%) were non-Hispanic white. More than half (53%) sought testing because of COVID-19 symptoms. Of those who tested positive, 66% reported having come into close contact with a COVID-19 case, and 64% reported that those contacts were family members, compared with 15% of contacts who were schoolmates and 27% who were child care classmates.
School Attendance Was Not Found to Increase Likelihood Of Testing Positive
Attending in-person school or child care during the 2 weeks before the SARS-CoV-2 test was not associated with greater likelihood of testing positive, the study authors noted, adding that the majority of study respondents reported universal mask use inside school and child care facilities, consistent with Mississippi State Department of Health recommended guidelines.
False reports of a new ‘U.S. variant’ originated from Dr. Deborah Birx on the task force. – New York Times
Reports of a highly contagious new variant in the United States, published on Friday by multiple news outlets, are based on speculative statements made by Dr. Deborah Birx and are inaccurate, according to several government officials.
The erroneous report originated at a recent meeting where Dr. Birx, a member of the White House coronavirus task force, presented graphs of the escalating cases in the country. She suggested to other members of the task force that a new, more transmissible variant originating in the U.S. might explain the surge, as another variant did in Britain.
Her hypothesis made it into a weekly report sent to state governors. “This fall/winter surge has been at nearly twice the rate of rise of cases as the spring and summer surges. This acceleration suggests there may be a USA variant that has evolved here, in addition to the UK variant that is already spreading in our communities and may be 50% more transmissible,” the report read. “Aggressive mitigation must be used to match a more aggressive virus.”
Dismayed, officials at the C.D.C. tried to have the speculative statements removed, but were unsuccessful, according to three people familiar with the events.
Dismayed, officials at the C.D.C. tried to have the speculative statements removed, but were unsuccessful, according to three people familiar with the events.
C.D.C. officials did not agree with her assessment and asked to remove it but were told no, according to one frustrated C.D.C. official, speaking on condition of anonymity for fear of retaliation.
Dr. Birx could not immediately be reached for comment.
The news of a possible new variant first appeared Friday afternoon on CNBC, quickly spread to other outlets. Responding to media inquiries about the variant, the C.D.C. issued a formal statement refuting the theory.
[editor’s note: also read There is no evidence homegrown variant is fueling coronavirus surge in the US, CDC says]
Moderna believes the second dose of its Covid-19 vaccine can be effectively administered between 21 to 42 days after the first dose, Ray Jordan, a spokesperson for the company, told CNN Friday.
Moderna declined to say whether the company could meet demand for second doses of coronavirus vaccine if the incoming Biden administration releases all vaccine at once, instead of holding back half.
In clinical trials, Moderna’s vaccine was given as two doses 28 days apart. On Friday, President-elect Joe Biden’s team said his administration would release all doses of coronavirus vaccines right away, instead of holding back half to ensure second doses are given on time, as the Trump administration has been doing.
When asked if Moderna would be able to produce enough additional vaccine to get second doses administered on day 28, the company declined to directly answer.
“Moderna is not aware of changed requirements associated with the Biden plan but has affirmed its plan to deliver according to the existing government supply contracts,” Jordan said. “This includes an expectation of delivering 100 million doses by the end of the first quarter and 200 million doses total by the end of the second quarter. Earlier this week, Moderna reported having already delivered 18 million doses to the US government.”
The World Health Organization’s vaccine advisers said earlier Friday that the second dose of Pfizer’s vaccine could also be administered as long as 42 days – six weeks – after the first dose.
What the data show about allergic reactions to COVID-19 vaccines – National Geographic
As vaccination efforts against COVID-19 haltingly ramp up across the United States, the country’s public health officials are confirming that severe allergic reactions to the Pfizer-BioNTech COVID-19 vaccine are rare.
In a study released January 6 by the U.S. Centers for Disease Control and Prevention (CDC), researchers revealed that the risk of anaphylaxis—a severe, potentially life-threatening allergic reaction—from the vaccine is extremely low. Based on data from people who have received the first of the two recommended doses, only about one in every 90,000 people, on average, will experience this adverse reaction. That’s less than 3 percent of the lifetime risk of dying from choking on food.
Technically, the chance of severe allergic reactions from the Pfizer-BioNTech vaccine is about 8.5 times higher than the risk from the seasonal flu vaccine, which has a rate of about one in 769,000. But experts point out it’s still a tiny number: According to the study, 1.89 million people in the U.S. received the first dose of the vaccine between December 14 to December 23, and more than 99.998 percent of them did not experience anaphylaxis.
Overall, though, the data reveal that the risk of anaphylaxis is far smaller than the negative outcomes associated with COVID-19 infections, especially among older Americans. By October 2020, the disease had become one of the leading causes of death in the U.S. among people more than 45 years old, outpacing automotive collisions, suicide, homicide, and accidental drug overdoses. To date, the pandemic has killed more than one out of every 1,000 Americans.
“I and my colleagues at CDC and FDA are committed to ensuring that COVID-19 vaccines are safe,” Nancy Messonnier, director of the CDC’s National Center for Immunization and Respiratory Diseases, said in a Wednesday press briefing on the study. “I know I look forward to the day I get to roll up my sleeve and get vaccinated.”
… To ensure a swift response in case of a rare allergic reaction, people will need to be observed for 15 minutes after getting the vaccine. People with a history of anaphylaxis or immediate allergic reactions will need to be monitored for 30 minutes.
Clark outlined two specific examples of people who should not get the full two-dose Pfizer-BioNTech vaccine regimen: “If you had an immediate reaction to your first [COVID-19 vaccine] dose, don’t get a second, and if you have a known allergy to components in the vaccine, or very closely related compounds, we recommend you not get vaccinated at this time.” People who are unsure whether they may be allergic to a vaccine ingredient should speak to their doctors before vaccination.
Specifically, the CDC cautions that COVID-19 vaccines that use messenger RNA (mRNA)—including the Pfizer BioNTech and Moderna vaccines—also contain polyethylene glycol to shield the mRNA, so people with allergies to the compound shouldn’t get the vaccine. Likewise, people allergic to polysorbates—which chemically resemble polyethylene glycol—shouldn’t get the shot at this time.
No Need to Stop RAS Inhibitors in COVID-19 – MedPage
Hospitalized COVID-19 patients may safely continue taking their angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs), according to the small REPLACE COVID trial.
The study’s primary hierarchical endpoint — a global rank score in which patients were ranked by the severity of their COVID disease course according to various biomarkers and clinical events, with a lower rank score meaning more severe COVID-19 hospitalization — was about the same whether people were randomized to continue or discontinue these common blood pressure medications (median rank 73 vs 81, β-coefficient 8, 95% CI -13 to 29).
Continuation and discontinuation groups also showed no differences in the secondary endpoints of:
- All-cause death: 15% vs 13% (P=0.99)
- At least one adverse event: 39% vs 36% (P=0.77)
- Length of hospitalization: 6 vs 5 days (P=0.56)
The REPLACE COVID results were reported by Julio Chirinos, MD, PhD, of the University of Pennsylvania in Philadelphia, and colleagues, and published online in The Lancet Respiratory Medicine.
“Consistent with current international society recommendations, providers should continue to prescribe these medications in patients admitted to hospital with COVID-19 unless there is a distinct medical contraindication to ongoing therapy,” the trialists concluded.
Pfizer says its vaccine works against one of the key mutations in the variants found in Britain and South Africa. – New York Times
Pfizer and BioNTech announced on Friday that their vaccine is effective against one of the mutations present in the new contagious variants identified in Britain and South Africa.
The study was posted online Thursday night on the web site Biorxiv. It has not yet gone through formal scientific review.
Independent experts said the findings are good news, but cautioned that each of the variants has several other potentially dangerous mutations that have not yet been investigated. So it’s possible that one of those mutations affects how well the vaccine works.
“It’s the first step in the right direction,” said Dr. John Brooks, the chief medical officer for the Centers for Disease Control Covid-19 emergency response. “I’m hoping that the additional work that comes out in the future will fall in line with that finding.”
The following are foreign headlines with hyperlinks to the posts
More than 17 million people near Beijing are under stay-at-home orders.
Maker of Russia’s Sputnik V vaccine applies for emergency use authorization in the Philippines
Canadian prime minister anticipates “tough” days ahead as country considers extended lockdowns
The following additional national and state headlines with hyperlinks to the posts
Gavin Newsom Promises 1 Million Vaccines in 9 Days During CA COVID-19 Surge
Nurse Who Got COVID After First Vaccine Dose Had ‘False Sense of Security’
New York will start allowing essential workers and those over 75 to get a vaccine.
One university’s strategy for keeping coronavirus numbers down? Fill vending machines with tests.
The E.U. secures 300 million more doses of the Pfizer-BioNTech vaccine.
Some health officials have turned to Eventbrite to schedule vaccinations.
Los Angeles County hospitals prepare to ration care as Covid-19 cases overwhelm
Some independent US health care workers are struggling to get Covid-19 vaccines, AMA warns
Oregon using National Guard to speed up Covid-19 vaccination effort
CDC director warns of Covid-19 surge after US Capitol riot
Second coronavirus vaccine dose is “absolutely critical,” Fauci says
Nearly 6.7 million people vaccinated against coronavirus, CDC says
Some states have tapped dentists, retired physicians and medical students to administer vaccines
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
November 2020 Consumer Credit Expands But Is In Contraction If Student Loans Are Ignored
World Economy To Trail Pre-Pandemic Trajectory For Years
America’s Scariest Charts 05 January 2021
Warning to Readers
The amount of politically biased articles on the internet continues to increase. And studies and opinions of the experts continue to contradict other studies and expert opinions. Honestly, it is difficult to believe anything anymore. A study usually cannot establish cause and effect – but only correlation. Be very careful what you believe about this pandemic.

I assemble this coronavirus update daily – sifting through the posts on the internet. I try to avoid politically slanted posts (mostly from CNN, New York Times, and the Washington Post) and can usually find unslanted posts on that subject from other sources on the internet. I wait to publish posts on subjects that I cannot validate across several sources. But after all this extra work, I do not know if I have conveyed the REAL facts. It is my job to provide information so that you have the facts necessary – and then it is up to readers to draw conclusions.
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19 when recovering from COVID-19. Herd immunity does not look like an option without immunization although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a significantly higher death rate as there is relatively few hospitalizations and deaths in younger age groups..
- There are at least 8 strains of the coronavirus. New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
What we do or do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work.
- Do we develop lasting immunity to the coronavirus? Another coronavirus – the simple cold – does not develop long term immunity. However, How Many Americans Are Immune From COVID? Research into the coronavirus is running way behind the need for answers. Whilst we strive for herd immunity through vaccination – we lack an understanding of the general immunity people might have to the pandemic. This will affect the point herd immunity can be reached. The following articles discuss immunity: Can the Common Cold Help Protect You from COVID-19?, Does the Common Cold Protect You from COVID-19?, Immune cells for the common cold may recognize SARS-CoV-2
- To what degree do people who never develop symptoms contribute to transmission? Research early in the pandemic suggested that the rate of asymptomatic infections could be as high as 81%. But a meta-analysis, which included 13 studies involving 21,708 people, calculated the rate of asymptomatic presentation to be 17%.
- The accuracy of rapid testing is questioned – and the more accurate test results are not being given in a timely manner.
- Can children widely spread coronavirus? [current thinking is that they are a minor source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- Air conditioning contributes to the pandemic spread.
- It appears that there is increased risk of infection and mortality for those living in larger occupancy households.
- Male patients have almost three times the odds of requiring intensive treatment unit (ITU) admission compared to females.
- Outdoor activities seem to be a lower risk than indoor activities.
- Will other medical treatments for Covid-19 ease symptoms and reduce deaths? So far only remdesivir, Bamlanivimab,
and Regeneron) are approved for treatment. What drugs work?
Arthritis drugs tocilizumab and sarilumab could cut relative risk of death of those in intensive care by 24%
- A current scientific understanding of the way the coronavirus works can be found [here].
There is now a vaccine available – the questions remain:
- how effective it will be in the general population,
- will there be any permanent side effects that will appear months from now,
- how long immunity will last [we can currently say we do not know if it will last more than 4 months],
- there is no evidence the vaccine will block transmission
Heavy breakouts of coronavirus have hit farmworkers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>





