
Written by Steven Hansen
The U.S. new cases 7-day rolling average is 9.6 % LOWER than the 7-day rolling average one week ago. U.S. hospitalizations due to COVID-19 are now 3.9 % HIGHER than the rolling average one week ago. U.S. deaths due to coronavirus are now 8.5 % LOWER than the rolling average one week ago. Today’s posts include:
- U.S. Coronavirus New Cases are 227,315
- U.S. Coronavirus hospitalizations are at a record 125,379 (for the next 9 days this is the number to watch as new cases and deaths will not be accurately reported)
- U.S. Coronavirus deaths are at an elevated 3,419
- U.S. Coronavirus immunizations have been administered to 0.8% of the population
- The 7-day rolling average rate of growth of the pandemic shows new cases worsened, hospitalizations unchanged, and deaths worsened
- Florida Becomes 3rd U.S. State To Identify New Coronavirus Variant
- The Mutated Virus Is a Ticking Time Bomb
- New Covid-19 Strains: What Scientists Know About Coronavirus Variant
- US debates whether UK approach is better on COVID-19 vaccinations
- Pfizer Criticizes Sudden Change in Coronavirus Vaccine Dosing Regime in the U.K.
- Face Masks Protect Wearers, Others From COVID
- Moderna’s COVID-19 Vaccine Efficacy Confirmed in NEJM Study
- HHS announces action to protect distilleries from surprise $14K fee

The recent worsening of the trendlines for new cases should be attributed to going back to college/university, cooler weather causing more indoor activities, possible mutation of the virus, fatigue from wearing masks / social distancing, holiday activities, political rallies / voting, and continued loosening of regulations designed to slow the coronavirus spread.
My continuing advice is to continue to wash your hands (especially after using the toilet as COVID first sheds in your stool), putting down the toilet seat (as flushing the toilet releases a plume), wear masks, avoid crowds, and maintain social distancing. No handwashing, mask, or social distancing will guarantee you do not get infected – but it sure as hell lowers the risk in all situations – and the evidence to-date shows a lower severity of COVID-19. In addition, certain activities are believed to carry higher risk – like being inside in air conditioning and removing your mask (such as restaurants, around your children/grandchildren, bars, and gyms). It is all about viral load – and outdoor activities are generally safe if you can maintain social distance. Finally, studies show eating right (making sure you are supporting your immune system) and adequate sleep increase your ability to fight off COVID.
include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus1.htm’); ?>
Hospitalizations (grey line) and Mortality (green line)
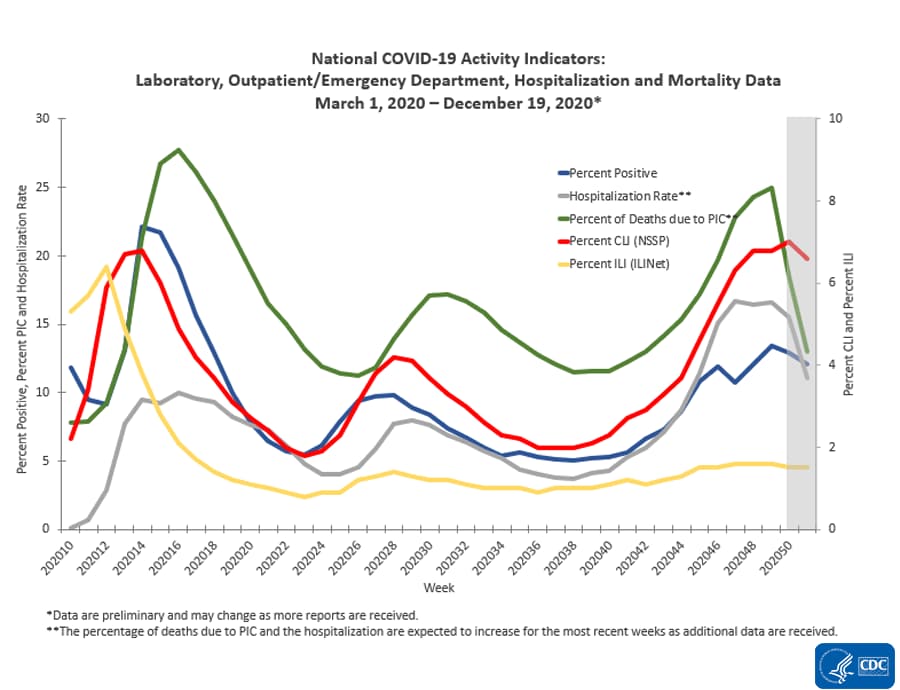
source: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html
The Impact of Holidays – Hospitalizations Are The Only Accurate Gauge As Most Reporting Is Not Timely
The 4 day Thanksgiving holiday period put a wobble in the trends. Over weekends and holidays, the number of new cases and deaths decline. Over weekends, this is not a problem for week-over-week rolling averages as weekends are compared against the previous weekend. But when a holiday falls within a working week, a non-working day is compared to a working day which causes havok in the trends. Now we are faced with the end of the year holiday season which means reporting is sporadic and numbers will initially look good – and then as the holidays end and the reporting catches up, the numbers will look terrible. In addition, family gatherings and travel will cause more virus transmission.
However, hospitalizations historically appear to be little affected by weekends or holidays – the daily counts do not vary significantly from day-to-day.
The hospitalization growth rate trend is growing at an ever slowing growth rate which is all good news as it means the number of beds needed is currently growing around 4 % every week.

The above graph demonstrates in the last week hospitalization rate of growth has been relatively steady. We have seen that the size of the impact of commingling and travel over the Thanksgiving holiday period – roughly, it seems to have added around 5 % to the rate of growth of new cases, hospitalizations, and deaths.
Historically, hospitalization growth follows new case growth by one to two weeks.
As an analyst, I use the rate of growth to determine the trend. But, the size of the pandemic is growing in terms of real numbers – and if the rate of growth does not become negative – the pandemic will overwhelm all resources.
The graph below shows the rate of growth relative to the growth a week earlier updated through today [note that negative numbers mean the rolling averages are LOWER than the rolling averages one week ago]. As one can see, the rate of growth for new cases peaked in early December 2020 ago and the rate of growth has been decelerating since.

This graph is currently demonstrating that the actions to contain the pandemic are slightly working – but the rate of growth improvement is too slow as we are still seeing some record numbers. In the scheme of things, new cases decline first, followed by hospitalizations, and then deaths.
It is up to each of our readers to protect themselves and others by washing your hands, wearing a mask, avoiding crowds, and maintaining social distancing.
Likely There Will Be A Pandemic Surge After New Years
The “experts” will tell you they told you so – and you should have stayed at home instead of traveling to be with the people you care about. And there is some truth in this opinion.
But there will be no way to accurately understand the impact of the holidays because there are new mutant strains of the coronavirus that are more transmissible.
To gauge the impact of anything, you change ONLY ONE variable at a time (and hopefully in a controlled environment). There are now two variables in play – and it is nearly impossible to separate the impact of each.
Coronavirus News You May Have Missed
Florida Becomes 3rd U.S. State To Identify New Coronavirus Variant – NPR
Florida is the third U.S. state to announce it has a case of the more contagious coronavirus strain that first emerged in the United Kingdom.
A man in his 20s, with no history of travel, tested positive for the mutated coronavirus. The state Department of Health said he is in Martin County.
The man’s diagnosis follows a similar case identified in California on Wednesday in which a male patient, also in his 20s, had not spent any time outside of the U.S. in the weeks prior to his illness.
The first two cases in the U.S. also adhere to that pattern. Two male members of the Colorado National Guard tested positive for the new strain — referred to as B.1.1.7 or VUI-202012/01 — and neither reported international travel. At least one of the two men is in his 20s.
Florida officials said they are working with the Centers for Disease Control and Prevention to investigate the case.
HHS announces action to protect distilleries from surprise $14K fee – The Hill
The Department of Health and Human Services (HHS) on Thursday said it is taking action to prevent distilleries that produce hand sanitizer during the pandemic from being hit with an unexpected $14,000 fee.
The move comes two days after the Food and Drug Administration (FDA) said that any distillery that had switched to producing hand sanitizer during the pandemic this year would owe thousands of dollars in fees, and could be charged twice if they do not cease production immediately.
Many craft-brewing distilleries switched production to non-consumable alcohol in response to the COVID-19 pandemic and a shortage of the product’s availability in the spring.
HHS officials said they first became aware of the fees this week and held an emergency meeting in response. They later instructed the FDA not to collect the fees.
“Small businesses who stepped up to fight COVID-19 should be applauded by their government, not taxed for doing so. I’m pleased to announce we have directed FDA to cease enforcement of these arbitrary, surprise user fees. Happy New Year, distilleries, and cheers to you for helping keep us safe!” an HHS spokesman said in a statement provided to The Hill.
Moderna’s COVID-19 Vaccine Efficacy Confirmed in NEJM Study – Medscape
The recently authorized COVID-19 vaccine developed by Moderna and the National Institute of Allergy and Infectious Diseases (NIAID) was 94.1% effective in preventing symptomatic COVID-19, according to phase 3 trial results published December 30 in The New England Journal of Medicine.
No cases of severe COVID-19 occurred among participants who received the vaccine, known as mRNA-1273, and there were no safety concerns.
The US Food and Drug Administration on December 18 issued an emergency use authorization for the vaccine, a lipid-nanoparticle-encapsulated mRNA vaccine expressing the prefusion-stabilized spike glycoprotein.
The trial began in July and enrolled 30,420 adults in the United States. Volunteers were randomly assigned in a 1:1 ratio to receive either two doses of the vaccine or two shots of saline placebo 28 days apart. The average age of the participants was 51 years.
In all, 196 cases of symptomatic COVID-19 occurred at least 14 days after participants received their second shot — 185 cases in the placebo group, and 11 in the vaccine group.
In a secondary analysis that included cases that occurred at least 14 days after the first shot, vaccine efficacy was 95.2%, study author Lindsey R. Baden, MD, of Brigham and Women’s Hospital, Boston, Massachusetts, and colleagues report.
Face Masks Protect Wearers, Others From COVID – Reuters
Two new literature reviews suggest face masks provide some protection to the wearer and when universally worn by the general public they substantially reduce the spread of the new coronavirus.
The reviews, published in Annals of Internal Medicine, look specifically at the effect of masking on COVID-19 transmission.
One report analyzed the impact of masking by the general public on the spread of the virus. Researchers reviewed over 100 research articles and concluded that masking could substantially reduce the spread of viruses, including SARS-CoV-2, without risks to the wearer.
“Our review clearly shows that masks and face coverings worn by members of the public are highly effective in reducing the spread of SARS-CoV-2,” said study leader Dr. Thomas Czypionka, head of the Health Economics and Health Policy Unit at the Institute for Advanced Studies in Vienna, Austria and visiting senior research fellow at the London School of Economics and Political Science.
“A growing body of evidence suggests that the virus is transmitted through drops in close contact situations and through aerosols, small particles hovering in the air for extended periods of time that accumulate especially in closed and crowded spaces,” Dr. Czypionka said in an email. “Such situations should be avoided of course, but if you can’t – for example, on public transport, in shops etc. – masks and face coverings can substantially reduce the risk of infection, mainly by source control, that is, by trapping the particles exhaled. There is also laboratory evidence that they may protect the wearer as well. Therefore, masks can literally save lives, and in a situation like this, with community spread, they should be widely used.”
There are many misconceptions about masks, Dr. Czypionka said. “One is that they lead to physiological changes like elevated carbon dioxide levels or decreased oxygen levels in the blood,” he added. “Masks and face coverings may cause discomfort for some people, but we found no empirical evidence for masks to cause harm.”
The second report — an update to a “living review” of data on mask use by the general public and by health care workers — focused mainly on three studies: one study of masking and the prevention of SARS-CoV-2 in a community setting (the DANMASK trial) and two studies of mask use in healthcare settings.
The DANMASK open label trial, which included 6,024 community dwelling adults in Denmark, found that the incidence of SARS-CoV-2 infection among participants was 2%. Surgical mask use as compared to no mask use was associated with a small reduction in risk for infection, but the finding was not statistically significant, the researchers noted.
“The study suggests that masks may have small benefits in reducing the risk of infection in the wearer,” said the report’s lead author, Dr. Roger Chou, a professor in the School of Medicine at the Oregon Health and Sciences University.
The Mutated Virus Is a Ticking Time Bomb – The Atlantic
There is much we don’t know about the new COVID-19 variant—but everything we know so far suggests a huge danger.
Anew variant of the coronavirus is spreading across the globe. It was first identified in the United Kingdom, where it is rapidly spreading, and has been found in multiple countries. Viruses mutate all the time, often with no impact, but this one appears to be more transmissible than other variants—meaning it spreads more easily. Barely one day after officials announced that America’s first case of the variant had been found in the United States, in a Colorado man with no history of travel, an additional case was found in California.
There are still many unknowns, but much concern has focused on whether this new variant would throw off vaccine efficacy or cause more severe disease—with some degree of relief after an initial study indicated that it did not do either. And while we need more data to feel truly reassured, many scientists believe that this variant will not decrease vaccine efficacy much, if at all. Health officials have started emphasizing the lack of evidence for more severe disease.
All good and no cause for alarm, right? Wrong.
A more transmissible variant of COVID-19 is a potential catastrophe in and of itself. If anything, given the stage in the pandemic we are at, a more transmissible variant is in some ways much more dangerous than a more severe variant. That’s because higher transmissibility subjects us to a more contagious virus spreading with exponential growth, whereas the risk from increased severity would have increased in a linear manner, affecting only those infected.
Increased transmissibility can wreak havoc in a very, very short time—especially when we already have uncontrolled spread in much of the United States. The short-term implications of all this are significant, and worthy of attention, even as we await more clarity from data. In fact, we should act quickly especially as we await more clarity—lack of data and the threat of even faster exponential growth argue for more urgency of action. If and when more reassuring data come in, relaxing restrictions will be easier than undoing the damage done by not having reacted in time.
To understand the difference between exponential and linear risks, consider an example put forth by Adam Kucharski, a professor at the London School of Hygiene & Tropical Medicine who focuses on mathematical analyses of infectious-disease outbreaks. Kucharski compares a 50 percent increase in virus lethality to a 50 percent increase in virus transmissibility. Take a virus reproduction rate of about 1.1 and an infection fatality risk of 0.8 percent and imagine 10,000 active infections—a plausible scenario for many European cities, as Kucharski notes. As things stand, with those numbers, we’d expect 129 deaths in a month. If the fatality rate increased by 50 percent, that would lead to 193 deaths. In contrast, a 50 percent increase in transmissibility would lead to a whopping 978 deaths in just one month—assuming, in both scenarios, a six-day infection-generation time.
Transmissibility increases can quickly—very quickly—expand the baseline: Each new infected person potentially infects many more people. Severity increases affect only the infected person. That infection is certainly tragic, and this new variant’s lack of increase in severity or lethality thankfully means that the variant is not a bigger threat to the individual who may get infected. It is, however, a bigger threat to society because it can dramatically change the number of infected people. To put it another way, a small percentage of a very big number can easily be much, much bigger than a big percentage of a small number.
[editor’s note: this is a long article which deserves a full read]
New Covid-19 Strains: What Scientists Know About Coronavirus Variants – Wall Street Journal
Scientists around the world are scrambling to learn more about previously unknown variants of the coronavirus that seem to spread from person to person more readily than other versions of the Covid-19-causing pathogen.
One new variant, known as B.1.1.7, was identified in December in the U.K., leading to travel restrictions and a widespread lockdown there. Since then, the U.K. variant has been detected in China and other countries, as well as in Colorado, California and Florida.
… Some doctors worry that the new variants of the coronavirus could supercharge the spread of Covid-19, putting additional stress on hospitals and nursing homes when cases are near their historic highs.
Preliminary data suggest that the new variants are no more likely to cause severe illness than the more familiar forms of the coronavirus. But even if their virulence isn’t greater, the variants’ apparently increased transmissibility could spell more misery and death by increasing the number of cases of Covid-19.
Researchers from the London School of Hygiene and Tropical Medicine combined behavioral and epidemiological data on patterns of disease transmission with mathematical models to determine whether the U.K. variant is more transmissible than previously identified variants.
They found the new variant to be more transmissible than previous variants.
… Is it possible that the rapid spread of the new variants isn’t a result of increased infectiousness but instead of poor adherence to social distancing and other measures aimed at curbing contagion?
Scientists don’t think so, at least in the U.K. As evidence, Prof. Neil Ferguson, an epidemiologist at Imperial College London and a member of a scientific panel that advises the British government on respiratory-virus threats, pointed to epidemiological data from November showing that cases of the new U.K. variant were exploding in the area southeast of London as coronavirus cases were falling in other parts of the country. The entire country was in lockdown during this period.
The situation may be different in South Africa, where researchers said human behavior might be playing a key role in the surge of cases. Millions of South Africans traveled widely in recent weeks, and tens of thousands had gathered in restaurants and bars and on beaches during the holiday season.
… While there is no final word yet on whether the existing vaccine made by Pfizer Inc. and BioNTech SE and the one from Moderna Inc. confer immunity to the new variants, scientists have expressed confidence that they do.
The mutations “raise some questions about vaccine efficacy, but it’s important to note that the vaccines elicit a broad immune response…that targets several areas of the spike protein,” said Dr. Richard Lessells, an infectious-disease specialist at the University of KwaZulu-Natal in Durban, South Africa, and a member of the team that discovered the South African variant.
Pfizer and Moderna have conducted lab tests of their vaccines against several versions of the coronavirus and found that the vaccines were effective against all, according to the drugmakers. The companies said they were conducting experiments to determine whether antibodies generated by people vaccinated were effective against the U.K. and South Africa variants.
US debates whether UK approach is better on COVID-19 vaccinations – The Hill
A new approach to COVID-19 vaccination just adopted in the United Kingdom is gaining traction in America, but is dividing public health experts.
In an effort to push out as many doses of the vaccine as possible, British officials will no longer hold back the second of two doses.
Instead, they will prioritize giving people the first dose and delay the second shot for as long as three months.
“Everyone will still receive their second dose and this will be within 12 weeks of their first. The second dose completes the course and is important for longer-term protection,” the U.K. government said in a statement.
“With two vaccines now approved, we will be able to vaccinate a greater number of people who are at highest risk, protecting them from the disease and reducing mortality and hospitalization.”
Each of the two vaccines currently authorized for use in the U.S. require two doses, given either three or four weeks apart.
Under the current distribution plan, the administration’s Operation Warp Speed only delivers half the number of needed doses to states every week. The other half remain in a warehouse, held back to ensure there is enough supply for a second dose.
With the U.S. vaccination campaign crawling out of the gate and more than 3,000 people dying of COVID-19 every day, proponents of the British policy don’t understand why the administration isn’t using every single vaccine it has.
“Why not vaccinate as many people with a single dose as you possibly can, with the intention that you should backfill that second dose later?” said Christopher Gill, a professor of global health at the Boston University School of Public Health.
Pfizer Criticizes Sudden Change in Coronavirus Vaccine Dosing Regime in the U.K. – Motley Fool
The gap between the first and booster doses of Pfizer (NYSE:PFE) and BioNTech‘s (NASDAQ:BNTX) coronavirus vaccine has been widened substantially in the U.K. — and Pfizer is not pleased about it.
The U.K.’s joint committee on vaccination and immunization, an advisory body that advises government healthcare agencies, approved new dosing guidelines for both Pfizer/BioNTech’s BNT162b2 and the just-approved AZD1222 from AstraZeneca and the University of Oxford. The new guidelines state that both vaccines’ two requisite shots can be administered as much as three months apart.
The key aim of the new recommendation appears to be to get as many people inoculated as possible with the initial shot. Research indicates that partial protection against the coronavirus can start as soon as 12 days after the first jab.
However, according to the Financial Times, Pfizer said, “[Our] study … was designed to evaluate the vaccine’s safety and efficacy following a two-dose schedule, separated by 21 days … The safety and efficacy of the vaccine has not been evaluated on different dosing schedules, as the majority of trial participants received the second dose within the window specified in the study design.”
It also said that there is no data indicating the vaccine’s initial dose is effective after those 21 days.
The following are foreign headlines with hyperlinks to the posts
Belgian retirement home records 26 COVID-19 deaths after visiting Santa tests positive
Israel could become the first country to vaccinate all of its citizens.
Macron promises to speed up France’s vaccine rollout after frustration over sluggish start.
Thailand bans food, drink, newspapers and magazines on domestic flights
WHO approves Pfizer/BioNTech vaccine in breakthrough for developing nations
Coronavirus overshadows Japan’s New Year’s Day festivities
2020’s Bio-Economic World War: Communist China Lied; Millions Of Humans Died
The following additional national and state headlines with hyperlinks to the posts
Amid Health Care Worker Shortage, LA Mayor Presses For Faster Vaccine Rollout
TV Studios Delay Shooting Due to Spike In Los Angeles COVID Rates
Pharmacist Arrested For Destroying 570 Doses of COVID Vaccine
U.S. Surgeon General Makes Personal COVID Plea as Wife Admitted to Hospital
Georgia’s [Senator] David Perdue Quarantining After Being Near COVID-Positive Person
LA public health agency tweets COVID-19 death every 10 minutes to encourage people to stay home
The Navy base at Guantánamo Bay will receive its first batch of vaccines in January.
New Hampshire’s governor scraps his outdoor inauguration, citing threats from anti-mask protesters.
California hospitals stressed to the ‘brink of catastrophe’ by the coronavirus surge
El Paso teacher whose video of students hugging became a national sensation dies from Covid-19
US Rep. Gwen Moore said Monday that she has tested positive for Covid-19, becoming the latest member of Congress to announce they’ve contracted the virus.
SE Georgia woman survives 95 days in two hospitals, rehab centers battling COVID-19
Browns keep practice facility closed amid coronavirus concerns
Dr. Drew Pinsky, who apologized for downplaying coronavirus, says he has Covid-19
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
Rail Week Ending 26 December 2020 – Ends Year Improving
25 December 2020 ECRI’s WLI Growth Rate Continues To Improve
A Look At The Feds Emergency Lending Programs
Oxford COVID Vaccine Authorised In The UK – Global Health Expert On Why This Is A Key Moment
January 2021 Economic Forecast – Continuing A Weak But Improving Economy
Warning to Readers
The amount of politically biased articles on the internet continues to increase. And studies and opinions of the experts continue to contradict other studies and expert opinions. Honestly, it is difficult to believe anything anymore. A study usually cannot establish cause and effect – but only correlation. Be very careful what you believe about this pandemic.

I assemble this coronavirus update daily – sifting through the posts on the internet. I try to avoid politically slanted posts (mostly from CNN, New York Times, and the Washington Post) and can usually find unslanted posts on that subject from other sources on the internet. I wait to publish posts on subjects that I cannot validate across several sources. But after all this extra work, I do not know if I have conveyed the REAL facts. It is my job to provide information so that you have the facts necessary – and then it is up to readers to draw conclusions.
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19 when recovering from COVID-19. Herd immunity does not look like an option without immunization although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a significantly higher death rate as there is relatively few hospitalizations and deaths in younger age groups..
- There are at least 8 strains of the coronavirus. New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
What we do or do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work.
- Do we develop lasting immunity to the coronavirus? Another coronavirus – the simple cold – does not develop long term immunity. However, How Many Americans Are Immune From COVID? Research into the coronavirus is running way behind the need for answers. Whilst we strive for herd immunity through vaccination – we lack an understanding of the general immunity people might have to the pandemic. This will affect the point herd immunity can be reached. The following articles discuss immunity: Can the Common Cold Help Protect You from COVID-19?, Does the Common Cold Protect You from COVID-19?, Immune cells for the common cold may recognize SARS-CoV-2
- To what degree do people who never develop symptoms contribute to transmission? Research early in the pandemic suggested that the rate of asymptomatic infections could be as high as 81%. But a meta-analysis, which included 13 studies involving 21,708 people, calculated the rate of asymptomatic presentation to be 17%.
- The accuracy of rapid testing is questioned – and the more accurate test results are not being given in a timely manner.
- Can children widely spread coronavirus? [current thinking is that they are a minor source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- Air conditioning contributes to the pandemic spread.
- It appears that there is increased risk of infection and mortality for those living in larger occupancy households.
- Male patients have almost three times the odds of requiring intensive treatment unit (ITU) admission compared to females.
- Outdoor activities seem to be a lower risk than indoor activities.
- Will other medical treatments for Covid-19 ease symptoms and reduce deaths? So far only remdesivir, Bamlanivimab,
and Regeneron) are approved for treatment. What drugs work?
- A current scientific understanding of the way the coronavirus works can be found [here].
There is now a vaccine available – the questions remain:
- how effective it will be in the general population,
- will there be any permanent side effects that will appear months from now,
- how long immunity will last [we can currently say we do not know if it will last more than 4 months],
- there is no evidence the vaccine will block transmission
Heavy breakouts of coronavirus have hit farmworkers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>




