
Written by Steven Hansen
The U.S. new cases 7-day rolling average is 16.9 % HIGHER than the 7-day rolling average one week ago. U.S. deaths due to coronavirus are now 1.0 % HIGHER than the rolling average one week ago. U.S. hospitalizations due to COVID-19 are now 10.8 % HIGHER than the rolling average one week ago. Today’s headlines include:
- Rolling averages declined today after peaking during last week
- 7 ways to fix this pandemic — and stop the next one
- Dozens of COVID-19 vaccines are in development. Here are the ones to follow
- Europe Back in Lockdown Mode
- Nursing home residents continue to grapple with effects of isolation

The recent worsening of the trendlines for new cases should be attributed to going back to college/university, cooler weather causing more indoor activities, possible mutation of the virus, fatigue from wearing masks / social distancing, holiday activities, and continued loosening of regulations designed to slow the coronavirus spread.
My continuing advice is to continue to wash your hands, wear masks, avoid crowds, and maintain social distancing. No handwashing, mask, or social distancing will guarantee you do not get infected – but it sure as hell lowers the risk in all situations – and the evidence to-date shows a lower severity of COVID-19. In addition, certain activities are believed to carry higher risk – like being inside in air conditioning and removing your mask (such as restaurants, around your children/grandchildren, bars, and gyms). It is all about viral load – and outdoor activities are generally safe if you can maintain social distance.
include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus1.htm’); ?>
Hospitalizations (grey line) and Mortality (green line) For Week ending 24OCT2020
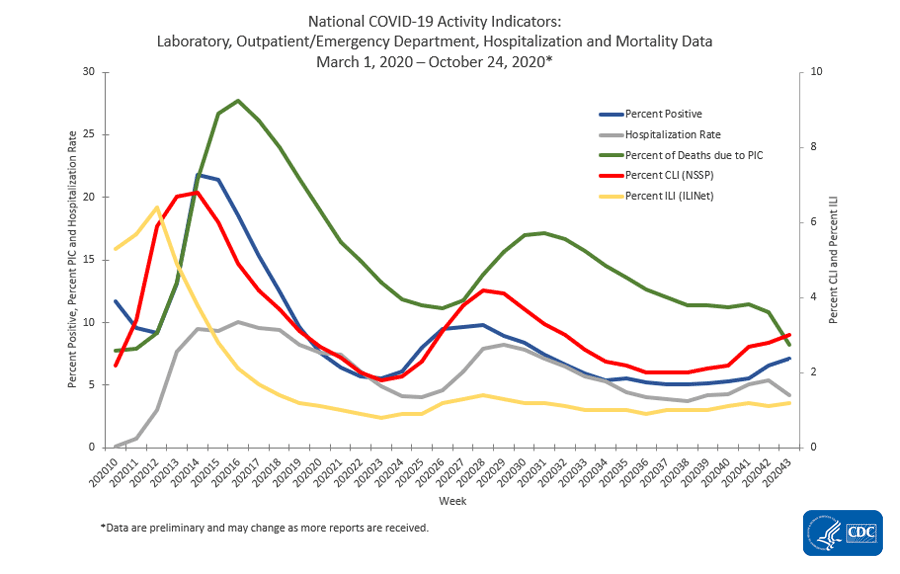
source: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html
The Coronavirus Is Not Going Away No Matter Who You Vote For
The more I study the coronavirus and listen to the “experts” – the more I am convinced COVID-19 is here to stay much like the common cold and the flu.
When this pandemic began, one fact kept hitting me in the face – there has never been a successful vaccine for immunity against a coronavirus. Case in point – the coronavirus which produces the common cold.
However, I believed that piggy-backing on the existing research into SARS (2002) and MERS (2012), there could be the foundation for the development of an effective vaccine for COVID-19. Neither SARS nor MERS infections were widespread – so the pharmaceutical companies could not afford to throw a lot of money at developing a vaccine.
Unlike SARS and MERS, COVID-19 is widespread, and a successful vaccine would be a goldmine to the pharmaceutical company which finds the “cure”. Potential profits, I believed, would be a large enough driver for the development of a successful vaccine.
But Dr. Fauci doused that hope in early August saying:
We don’t know yet what the efficacy might be. We don’t know if it will be 50 percent or 60 percent. I’d like it to be 75 percent or more. But the chances of it being 98 percent effective is not great, which means you must never abandon the public health approach.
Another nail in the coffin for an effective vaccine was that immunity to the virus is shortlived following recovery – again, just like the common cold or the flu where a truly effective vaccine does not exist.
The final nail in the coffin is that only around half of Americans would not take a COVID shot if one was available. This translates to literally half the population having no immunity even if the vaccine efficacy was 100%. But a 50% efficacy leaves 3/4’s of the population without immunity even with a vaccine. That is not even close to the immunity levels needed to stop this pandemic.
So where do we go from here?
- There must be an instantaneous home test for coronavirus – it defies logic that an affected person has to go out to be tested risking the lives of health care workers and others who have to come in contact with the affected person. The government needs to throw money to make this home test widely available so the average Joe has a test kit in their medicine cabinet. Why have not the “experts” pushed and spent money to make this happen?
- I would be throwing government money on developing an effective treatment – similar to the money being thrown to develop a vaccine. If it is here to stay, let’s work on solutions to avoid hospitalizations and deaths. All the “experts” seem to be doing is pushing currently available drugs that were not designed with the coronavirus in mind.
- Further to the effective treatment, I want to be able to go to Walmart, CVS, Walgreens, et al and buy the effective treatment off the shelf WITHOUT A PRESCRIPTION just like you do when you contract the common cold or flu.
- Lockdowns are measures of last resort – the “Hail Mary” if things get crazy. Little good comes out of partial or complete lockdowns – but it is the only option if the healthcare system gets overwhelmed. The populations in the lower quartiles of the economy must work as there are little savings to fall back on – and lockdowns take away their jobs and income. In fact, there are literally hundreds of significant repercussions resulting from lockdowns. Lockdowns must be avoided. Experts must work at providing solutions to minimizing the risk to people who must leave their house!
- I am a firm believer in masks and social distancing – this has been shown to be the most effective solution that is available. I am supportive of a national mask mandate – but at the same time, I believe it is unconstitutional on a national level – but constitutional on a state level. In southern Florida, we have been under an uninterrupted mask mandate since April. Yet cases are increasing here likely caused in part by the exodus from other states – the roads here are full of out-of-state vehicles. The cloth masks the “experts” expect us to wear are nowhere near 100% efficient – and may only be 50 % at best. My priority would be to produce N95 masks for everyone to maximize the efficacy of wearing a mask. I wear an N95 mask as I have never believed a cloth mask was effective enough (although much better than nothing). Why are not the “experts” pushing N95 masks?
- We have 50 states – why don’t we experiment with each state doing something different so that we can OPTIMIZE solutions. We will never know what was the right path to take if everyone walks down the same path. Why are the “experts” pushing for a uniform national strategy – this approach is far from scientific and more Orwellian.
I am a pragmatist – and honestly do not believe the crap being thrown around by the experts and the politicians. I watch for things that work and do not work. No matter who gets elected on 03 November – the pandemic is not going away. We will either be ruled by the same mentality which killed the economy (like in places like my beloved San Francisco) or the tough guy mentality which is exasperating the outbreak. Either way, we lose because at this point the virus is in charge – and nothing will change that short of the virus miraculously disappearing or a miracle pill / vaccine appearing. There are no options because the experts are single-mindedly committed to a single path of creating a vaccine and locking us down when their approach is not working.
The ONLY moderating method to control the coronavirus, for the time being, is masks and social distancing – and that is not effective enough as evidenced by the increasing COVID-19 cases in southern Florida which has been under a continuous mask mandate for almost 7 months. Our experts and politicians have let us down. There is no science – only unsupported beliefs and extrapolations espoused by the experts. And the situation is not unique in the U.S. – I see the same thing in most other advanced economies.
Bummer.
Coronavirus News You May Have Missed
Econintersect has published two posts today summarizing the coronavirus news over the last week:
7 ways to fix this pandemic — and stop the next one – Knowable
It’s hard to imagine a time when we were scared about another contagious disease, but in 2003, many of us working in hospital preparedness were incredibly worried about SARS. Although the number of cases was initially low, some estimates show that 10 percent of infected patients died. When my colleagues and I at the Johns Hopkins Center for Health Security mapped out what widespread transmission of a SARS-like virus could look like in the US, it was terrifying.
Thankfully, we came to learn that SARS was really contagious only when patients were very sick, not when they were asymptomatic or had mild illness. The epidemic was brought under control in about six months, with only 8,098 cases worldwide; the US had only eight patients and zero deaths. As an internist and emergency physician who focuses on preparing for pandemics, I knew that we had dodged a bullet.
… The country must face all the mistakes it made with Covid-19 to mitigate the effects of the next pandemic. And there will be a next one: Climate change, population growth and poor environmental policies around the world have created an age of epidemics. When I think of all the steps we should have taken, and how many deaths could have been avoided, my head spins. But some lessons are crystal-clear.
- First and foremost, Americans need to embrace the fact that public health interventions such as social distancing, wearing masks and avoiding crowded indoor areas really work.
- Infectious disease experts must also get a better understanding of the asymptomatic spread of SARS-CoV-2.
- The US government needs greater control over the medical-supply chain.
- The US must create a high-level, permanent federal office with the authority, political power and budget to prepare for and immediately respond to catastrophic health emergencies, including pandemics.
- American hospitals need much more surge capacity.
- To mitigate the effect of any infectious disease, rapid testing that provides results in hours (or even minutes), not days, would make all the difference.
- Finally, the US suffers immensely without consistent leadership and communications.
Dozens of COVID-19 vaccines are in development. Here are the ones to follow. – National Geographic
More than 150 coronavirus vaccines are in development across the world—and hopes are high to bring one to market in record time to ease the global crisis.
COVAXIN (Bharat Biotech) – [preliminary results from early vaccine trials found more than 90 percent of human participants developed antibodies.] On October 23, Bharat Biotech announced it has received approval to start phase three trials in 26,000 participants at more than 25 centers across India.
Novavax – [the vaccine was safe and produced coronavirus antibodies at a higher level than is seen among those who have recovered from COVID-19. It also stimulated T cells, another arm of the human immune response.] phase three trial in the United Kingdom, which will evaluate the vaccine in up to 10,000 people, both with and without underlying conditions.
Johnson & Johnson – [a piece of DNA from SARS-CoV-2 into the common cold-causing adenovirus that has been genetically changed so that it can’t replicate in the body. This vaccine builds on the technology Johnson & Johnson used to develop an Ebola vaccine as well as vaccine candidates for Zika and HIV. In July, a study published in Nature showed that the vaccine elicited neutralizing antibodies in monkeys and provided “complete or near-complete” protection with just one dose] In a phase three ENSEMBLE trial to evaluate the safety of the vaccine—and how well it works—among up to 60,000 adults from a variety of countries.
Moderna Therapeutics – [vaccine candidate relies on injecting snippets of a virus’s genetic material, in this case mRNA, into human cells – Here’s how mRNA vaccines work.] Started the third phase of its clinical trials, even as it continues to monitor phase two results. Preliminary findings from phase one have shown that healthy subjects—including elderly patients—produced coronavirus antibodies and a reaction from T cells.
Pfizer – [Pfizer and BioNTech are also developing an mRNA vaccine based on the German company’s earlier efforts to use the technology in experimental cancer vaccines.] Preliminary results of phase one/two data show the vaccine produces antibodies and T-cell responses specific to the SARS-CoV-2 protein.
University of Oxford – [Oxford’s candidate is what’s known as a viral vector vaccine, essentially a “Trojan horse” presented to the immune system. Oxford’s research team has transferred the SARS-CoV-2 spike protein—which helps the coronavirus invade cells—into a weakened version of an adenovirus, which typically causes the common cold.] Preliminary results from this candidate’s first two clinical trial phases revealed that the vaccine had triggered a strong immune response—including increased antibodies and responses from T-cells—with only minor side effects such as fatigue and headache.
Sinovac- [CoronaVac is an inactivated vaccine that uses a non-infectious version of the coronavirus to provoke an immune response.] Preliminary results in macaque monkeys, published in Science, revealed that the vaccine produced antibodies that neutralized 10 strains of SARS-CoV-2.
Sinopharm – [Sinopharm is also using an inactivated SARS-CoV-2 vaccine that it hopes will reach the public by the end of 2020. Preliminary findings from two randomized trials, published in JAMA, have shown the vaccine can trigger an antibody response with no serious adverse effects.] On September 29, the New Yorker reported that Sinoparm is filing its application to China’s regulatory commission for approval of the vaccine, which could arrive sometime in October. The story also notes that hundreds of thousands of Chinese civilians have already been vaccinated under the government’s emergency-use approval.
Murdoch Children’s Research Institute – [For nearly a hundred years, the Bacillus Calmette-Guerin (BCG) vaccine has been used to prevent tuberculosis by exposing patients to a small dose of live bacteria. Evidence has emerged over the years that this vaccine may boost the immune system and help the body fight off other diseases as well.] In April, researchers from the Murdoch Children’s Research Institute began a series of randomized controlled trials that will test whether BCG might work on the coronavirus as well.
CanSino Biologics – [CanSino has also developed a viral vector vaccine, using a weakened version of the adenovirus as a vehicle for introducing the SARS-CoV-2 spike protein to the body.] Though the company was still technically in phase two of its trial, on June 25, CanSino became the first company to receive limited approval to use its vaccine in people. The Chinese government has approved the vaccine for military use only, for a period of one year.
Sputnik V – [a viral vector vaccine that also uses a weakened version of the common cold-causing adenovirus to introduce the SARS-CoV-2 spike protein to the body.] Despite the lack of published evidence, Russia has cleared the Sputnik V vaccine for widespread use and claimed it as the first registered COVID-19 vaccine on the market.
[editor’s note: this article deserves a full read as this is only a summary]
Europe Back in Lockdown Mode – Statista
As with the first set of lockdowns in the spring, the restrictions meant to curb the renewed spread of Covid-19 in Europe are happening fast and all at once.
Spain and France, where a second wave of infections spread from mid-July, led the way by imposing local lockdowns from early and mid-October, respectively. While France announced a national lockdown to start Friday, Spain’s local solution now includes several major provinces.
Germany is following these cues to lock down the country starting Nov. 2 (opting for the national route), while the UK introduced tiered, localized systems in England and Scotland, while Wales and Northern Ireland are already under lockdown.
The first second-wave lockdown in Europe actually started before the current rush – in Ireland, which has been under a nationwide lockdown since Oct 22.
Several more countries have introduced curfews to harness the spread of the coronavirus, forbidding their citizens to move around during night hours without a good reason. Spain is imposing this measure nationwide in addition to local lockdowns. National curfews are also in place in hard-hit Belgium as well as in Luxembourg, Slovenia and Slovakia.
Italy, faring better in the second wave, has so far only introduced localized curfews, but amended them with a nationwide mandatory closing hour for restaurants and bars that has been moved forward twice to an early 6 p.m. Restaurants are also shuttering early in Croatia and Denmark (among others), while they were forced to stop accepting all sit-in diners in the Netherland and Poland.
As with the first wave of lockdowns, enforcement varies significantly between countries, with Germany merely urging residents to stay at home, while more stringent checks are customary in Spain and France. Other then the first time around, several governments imposing restrictions have said that they are expecting to ease them again rather soon, starting in early December.
You will find more infographics at Statista

Nursing home residents continue to grapple with effects of isolation. – New York Times
The coronavirus continues to devastate long-term care facilities despite an array of safety measures and bans on visitors put in place months ago to slow the devastation.
More than 87,000 residents and workers have died of the virus, which has infected more than half a million people tied to the facilities. New clusters continue to erupt with numbing regularity: 16 people died this month at a nursing home in Chesterfield, Va.; all 62 residents of a nursing home in Kansas were infected.
At the same time, the damage of solitude is being overlooked, families and advocacy groups say. They say that widespread lockdowns are still necessary to protect people from the virus, but also that facilities must now confront a growing physical and mental toll of social isolation as the pandemic shows no sign of abating.
Separation from family and friends is among the hardest deprivations of the pandemic. Experts say the absence can inflict particularly serious damage on people with dementia and Alzheimer’s disease, thousands of whom have been confined to their buildings since March.
Operators of long-term care facilities say they are facing an impossible choice between depriving residents of vital human contact and inviting the virus inside.
The following are foreign headlines with hyperlinks to the posts
England tells residents to stay home, adding to Europe’s growing lockdowns.
Cases are rising in Russia’s far-flung provinces.
The following are additional national and state headlines with hyperlinks to the posts
Fauci Says Americans Should Expect ‘A Whole Lot of Hurt’ from COVID-19
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
Will Americans Go On A Spending Spree?
Growth Engines Not Yet In Sync: A Multispeed Recovery In Asia
Europe Needs To Maintain Strong Policy Support To Sustain The Recovery
Coronavirus Disease Weekly News 01November 2020
Coronavirus Economic Weekly News 01November 2020
The Scarring Effects Of Downturns On Young Workers
Warning to Readers
The amount of politically biased articles on the internet continues to increase. And studies and opinions of the experts continue to contradict other studies and expert opinions. Honestly, it is difficult to believe anything anymore. A study usually cannot establish cause and effect – but only correlation. Be very careful what you believe about this pandemic.

I assemble this coronavirus update daily – sifting through the posts on the internet. I try to avoid politically slanted posts (mostly from CNN, New York Times, and the Washington Post) and can usually find unslanted posts on that subject from other sources on the internet. I wait to publish posts on subjects that I cannot validate across several sources. But after all this extra work, I do not know if I have conveyed the REAL facts. It is my job to provide information so that you have the facts necessary – and then it is up to readers to draw conclusions.
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19. At this point, herd immunity does not look like an option although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a higher death rate.
- There are at least 8 strains of the coronavirus. New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
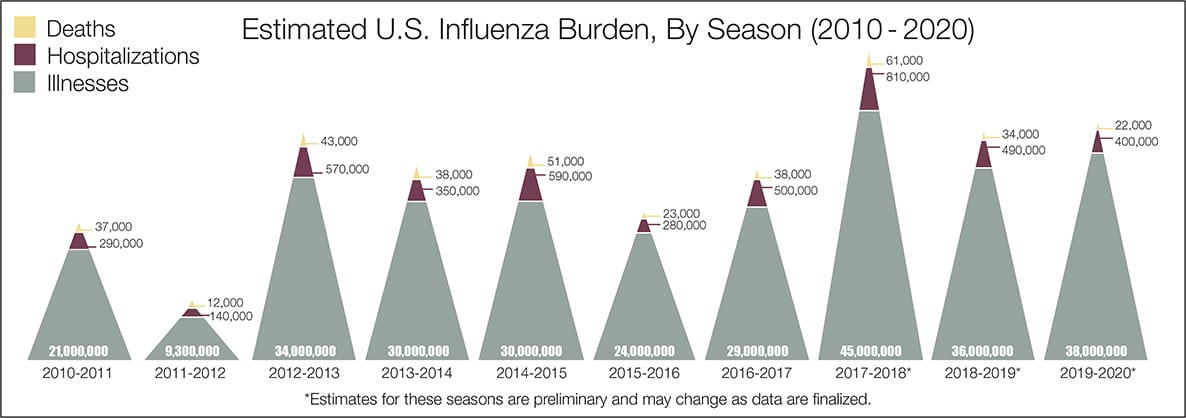
- The real question remains if the U.S. is over-reacting to this virus. The following graphic from the CDC puts the annual flu burden in perspective [click on image to enlarge]. Note that using this data is dangerous as the actual flu cases are estimated and not counted – nobody knows how accurate these guesses are.
What we do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work.
- Do we develop lasting immunity to the coronavirus? Another coronavirus – the simple cold – does not develop long term immunity.
- To what degree do people who never develop symptoms contribute to transmission?
- The US has scaled up coronavirus testing – and the accuracy of the tests has been improving. However, if one loses immunity – the coronavirus testing value is reduced.
- Can children widely spread coronavirus? [current thinking is that they are becoming a major source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- What effect will the weather have? At this point, it does not seem hot weather slows this coronavirus down – and it seems air conditioning contributes to its spread.
- Outdoor activities seem to be a lower risk than indoor activities.
- Can the world really push out an effective vaccine in 12 to 18 months?
- Will other medical treatments for Covid-19 ease symptoms and reduce deaths? So far only one drug (remdesivir) is approved for treatment.
- A current scientific understanding of the way the coronavirus works can be found [here].
Heavy breakouts of coronavirus have hit farm workers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of the respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>




