Written by Steven Hansen
The U.S. new cases 7-day rolling average is 10.5 % HIGHER than the 7-day rolling average one week ago. U.S. deaths due to coronavirus are now 8.4 % HIGHER than the rolling average one week ago. At the end of this post is a set of interactive graphs and tables for the world and individual States – as well as today’s headlines which include;
- Global daily new coronavirus cases continue at record levels
- The U.S. reported its second-highest daily case total since the start of the pandemic.
- Universal mask wearing could save 130,000 lives by spring
- FDA OKs Remdesivir, First Drug for COVID-19
- Moderna’s coronavirus vaccine trial is fully enrolled, 37 percent of participants are minorities
- Schoolchildren Seem Unlikely to Fuel Coronavirus Surges, Scientists Say
- Explaining declines in death rates from COVID-19
- Where Europe’s Second Wave Is Filling Up Hospitals
- For Covid-19 vaccine recipients, CDC to roll out cell phone-based monitoring system
- A new culprit for severe COVID-19 cases
- Hospital Bills For Uninsured COVID-19 Patients Are Covered, But No One Tells Them
- COVID-19 Plus Cancer Proves Deadly

The recent worsening of the trendlines for new cases should be attributed to going back to college/university, cooler weather causing more indoor activities, holiday activities, and continued loosening of regulations designed to slow the coronavirus spread.
My continuing advice is to continue to wash your hands, wear masks, and maintain social distancing. No handwashing, mask, or social distancing will guarantee you do not get infected – but it sure as hell lowers the risk in all situations – as the evidence to-date shows a lower severity of COVID-19. In addition, certain activities are believed to carry a higher risk – like being inside in air conditioning and removing your mask (such as restaurants, around your children/grandchildren, bars, and gyms). It is all about viral load – and outdoor activities are generally safe.
The daily number of new cases in the U.S. is remaining stubbornly and embarrassedly high – and is currently increasing.
The following graphs show the 7-day rolling average for new coronavirus cases and deaths have been updated through 23 October 2020:


z coronavirus.png
Hospitalizations (grey line) and Mortality (green line) For Week ending 17OCT2020
source: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html
Coronavirus Statistics For 23 October 2020 |
| U.S. Only | Global | U.S Percentage of Total | ||||
| Today*** | Cumulative | Today*** | Cumulative | Today | Cumulative | |
| New Confirmed Cases | 61,207 | 8,410,000 | 390,029 | 41,770,000 | 15.7% | 20.1% |
| Deaths** | 841 | 223,042 | 6,079 | 1,140,000 | 13.8% | 19.6% |
| Mortality Rate | 1.4% | 2.7% | 1.6% | 2.7% | ||
total COVID-19 Tests per 1,000 people | 2.23* | 415.63* | ||||
Source: EU CDC – The data insignificantly varies from the data produced by Johns Hopkins
* as of 20 Oct 2020
** evidently several States included “probable” deaths today in the number
*** red color indicates record number
Tracking Covid at U.S. Colleges and Universities
![]()
Coronavirus News You May Have Missed
Study: Universal mask wearing could save 130,000 lives by spring – Newsweek
Universal mask wearing could prevent nearly 130,000 deaths from COVID-19 through the end of February, according to new research released Friday.
The analysis, published in the journal Nature Medicine, found that even if only 85 percent of the population wore masks in public, nearly 96,000 lives could be saved.
But without universal masking, which the study defined as 95 percent compliance, more than a half a million lives could be lost to COVID-19, researchers at the Institute for Health Metrics and Evaluation (IHME) projected.
The most optimistic scientists do not predict the availability of new coronavirus treatments before 2021, and a vaccine might not be widely available until April at the earliest.
That means until there is a vaccine, masks and other non-pharmaceutical measures such as physical distancing are the only real ways to reduce transmission of the virus.
The findings match what public health officials have been saying for months, but mask wearing is still controversial. Only 49 percent of Americans said they always wear a mask in public.
FDA OKs Remdesivir, First Drug for COVID-19 – MedPage
The FDA approved remdesivir (Veklury) on Thursday for treating hospitalized COVID-19 patients, a first for the disease that started a global pandemic.
Remdesivir, an antiviral that works by limiting SARS-CoV-2 replication, is indicated for hospitalized patients age 12 and up (and at least 40 kg [88.2 lbs]). Previously, the intravenous drug was solely available under an emergency use authorization (EUA) from the agency.
FDA also announced a new EUA for remdesivir in hospitalized kids age 12 and older weighing at least 3.5 kg (7.7 lbs) but less than 40 kg, and in kids under age 12 weighing at least 3.5 kg.
The news comes exactly a week after a major international trial led by the World Health Organization (WHO) found no survival improvement for hospitalized COVID-19 patients treated with the drug, and no improvement in time to recovery.
Approval was based on three randomized trials, including the National Institutes of Health-led ACTT-1 trial, a phase III trial that showed that patients with mild, moderate, and severe disease who were treated with up to 10 days of remdesivir recovered a median 5 days quicker than those on placebo (10 vs 15 days; rate ratio [RR] 1.29, 95% CI 1.12-1.49, P<0.001), and a median 7 days quicker in those requiring oxygen at baseline (11 vs 18 days; RR 1.31, 95% CI 1.12-1.52).
Fewer patients on oxygen at baseline progressed to mechanical ventilation or extracorporeal membrane oxygenation with remdesivir (13% vs 23%), and a trend toward lower day-29 mortality was observed with the drug (11.4% vs 15.2%; HR 0.73, 95% CI 0.52-1.03).
Moderna’s coronavirus vaccine trial is fully enrolled, 37 percent of participants are minorities – Washington Post
Moderna, the biotechnology firm partnering with the National Institutes of Health to develop a coronavirus vaccine, announced Thursday that it has fully enrolled its trial, with 30,000 participants — more than a third of whom are minorities.
The coronavirus vaccine trials have been closely watched to ensure they reflect the diversity of the U.S. population at a minimum, and Moderna’s enrollment was slowed in September to recruit more minorities. A fifth of the participants are Hispanic and 10 percent are Black, according to data released by the company. People over 65, a population also at high risk for coronavirus, make up 25 percent of the study population.
“I think that we have done quite well — I think the demographics of the Moderna trial have markedly changed,” Larry Corey, a virologist at Fred Hutchinson Cancer Research Center said in an interview last week. Corey is heading up the clinical trials under Operation Warp Speed, the federal effort to speed vaccine development.
… Pharmaceutical giant Pfizer’s coronavirus vaccine trial is also nearing completion. Pfizer’s trial, which is not part of Operation Warp Speed, has enrolled 39,862 of its planned 44,000 participants. Of those, 34,601 have received their second, booster dose.
Half the participants in both trials receive the study vaccine and half receive a placebo, and more than 25,000 of Moderna’s participants have already received their second dose.
More than half of the volunteers in Moderna’s trial are healthy and not at high risk of severe covid-19, the disease caused by coronavirus. But 25 percent are at elevated risk due to age and 17 percent are younger, but have conditions such as diabetes or obesity that put them in a high risk group.
[editor’s note: also read Pfizer is including teens in its vaccine trials — a strategy some consider risky.]
For Covid-19 vaccine recipients, CDC to roll out cell phone-based monitoring system – CNN
Once a Covid-19 vaccine becomes available in the United States, the Centers for Disease Control and Prevention plans to monitor vaccine recipients for any health problems through text messages and online surveys, as part of a new program called V-SAFE.
“V-SAFE is a new smartphone-based active surveillance program for Covid-19,” Dr. Tom Shimabukuro, deputy director of the CDC’s Immunization Safety Office, said during a meeting of the US Food and Drug Administration’s Vaccines and Related Biological Products Advisory Committee on Thursday.
During the early phase of distributing a Covid-19 vaccine, initial doses may be given to specific groups, such as healthcare personnel and other essential workers, and so they likely would be the first to use V-SAFE. CNN has contacted the CDC for comment.
Through V-SAFE, which stands for “vaccine safety assessment for essential workers,” health checks can be conducted via text messages and email daily in the first week after a person receives the vaccine and then weekly thereafter for six weeks, according to the CDC’s website.
If a vaccine recipient reports any adverse events, the program will help submit a report to the US Department of Health and Human Services’ Vaccine Adverse Event Reporting System or VAERS.
“It includes active telephone follow-up,” Shimabukuro said. It’s a more active way to monitor for adverse events, instead of merely waiting for patients to report them.
Where Europe’s Second Wave Is Filling Up Hospitals – New York Times
… a second wave of serious illness is here, new data released on Thursday shows, making it clear that the pandemic is still dangerous and that adherence to control measures over the next few weeks will be crucial in preventing hospitals from becoming overrun for a second time this year.
Where People Are Sick From the Coronavirus
Patients in hospital per 100,000
Spring peak
% of spring peak
Czech Republic
35
4
882%
Spain
29
Belgium
22
50
43%
Bulgaria
21
6
381%
Poland
21
9
230%
Hungary
18
7
249%
France
16
48
34%
21 European countries
14
31
45%
Italy
13
55
24%
Slovenia
13
6
226%
Croatia
12
9
136%
Slovakia
12
4
285%
United States
11
18
61%
Portugal
11
13
83%
United Kingdom
10
30
33%
Austria
8
12
68%
Ireland
6
18
31%
Luxembourg
5
35
15%
Latvia
4
2
163%
Estonia
3
12
23%
Denmark
2
9
23%
Finland
1
4
23%
Norway
1
6
10%
Iceland
0.3
12
2%
Source: European Centre for Disease Prevention and Control. Hospital data for Europe includes 21 countries that report daily hospital occupancy data to the ECDC. Germany, the Netherlands and others are omitted. Spring peak is the highest value from March and April, except for Hungary where data collection began in May. Current patients in hospitals reflect the most recent available data.
The number of Covid-19 patients in hospitals across the continent is still less than half of the peak in March and April, but it is rising steadily each week, according to data from the European Centre for Disease Prevention and Control. People across much of Europe — including larger countries like France, Italy, Poland and Spain — are now more likely to be hospitalized with Covid-19 than those in the United States.
A new culprit for severe COVID-19 cases – DDN
More than 10 percent of people who develop severe COVID-19 have misguided antibodies that attack not the virus, but the immune system itself, new research shows. Another 3.5 percent, at least, carry a specific kind of genetic mutation.
In both groups, the upshot is basically the same: The patients lack type I interferon, a set of 17 proteins crucial for protecting cells and the body from viruses. Whether the proteins have been neutralized by so-called auto-antibodies, or were not produced in sufficient amounts in the first place due to a faulty gene, their missing-in-action appears to be a common theme among a subgroup of COVID-19 sufferers whose disease has thus far been a mystery.
Published in two papers in Science, the findings help explain why some people develop a disease much more severe than others in their age group—including, for example, individuals who required admission to the ICU despite being in their 20s and free of underlying conditions. They may also provide the first molecular explanation for why more men than women die from the disease.
“These findings provide compelling evidence that the disruption of type I interferon is often the cause of life-threatening COVID-19,” said Jean-Laurent Casanova, head of the St. Giles Laboratory of Human Genetics of Infectious Diseases at The Rockefeller University and a Howard Hughes Medical Institute investigator. “And at least in theory, such interferon problems could be treated with existing medications and interventions.”
The findings are the first results being published out of the COVID Human Genetic Effort, an ongoing international project spanning over 50 sequencing hubs and hundreds of hospitals around the world, co-led by Casanova and Helen Su at the National Institute of Allergy and Infectious Diseases. The study participants included various nationalities from Asia, Europe, Latin America, and the Middle East.
Study helps explain declines in death rates from COVID-19 – Medical Xpress
Fewer New Yorkers are dying from the coronavirus than health experts had anticipated, a new study shows. Regional death rates have dropped from the highs seen at the start of the outbreak, partially due to a shift in the population contracting the disease toward those who are more resilient.
After New York became the epicenter for the pandemic in early March, with tens of thousands dying from COVID-19, experts had expected that the infection would remain as deadly in the following months.
Instead, a new investigation showed that by mid-August the death rate in those hospitalized with coronavirus-related illness had dropped from 27 percentage points to about 3 percentage points. Led by researchers at NYU Grossman School of Medicine, the study showed that a younger, healthier group of people were getting infected and were arriving at the hospital with less-severe symptoms than those infected in the spring.
However, the researchers’ analysis showed that these factors accounted for only part of the improvement in survival. The rest, they suspect, resulted from health care providers‘ growing experience with the coronavirus. For example, physicians learned that resting COVID-19 patients on their stomachs rather than their backs and delaying the use of ventilators as long as possible were more effective practices, say the study authors. Drugs likely helped as well. In addition, other factors such as decreasing hospital volumes, less exposure to infection, and earlier testing and treatment, may have played a role.
“Our findings suggest that while COVID-19 remains a terrible disease, our efforts to improve treatment are probably working,” says study lead author Leora Horwitz, MD, an associate professor in the Department of Population Health at NYU Langone Health. “Even in the absence of a silver-bullet treatment or vaccine, we are protecting more of our patients through a host of small changes,” says Horwitz, who is also director of the Center for Healthcare Innovation and Delivery Science at NYU Langone.
Schoolchildren Seem Unlikely to Fuel Coronavirus Surges, Scientists Say – New York Times
So far, schools do not seem to be stoking community transmission of the coronavirus, according to data emerging from random testing in the United States and Britain. Elementary schools especially seem to seed remarkably few infections.
The evidence is far from conclusive, and much of the research has been tarnished by flaws in data collection and analysis. School reopenings are very much a work in progress. Still, many experts are encouraged by the results to date.
“The more and more data that I see, the more comfortable I am that children are not, in fact, driving transmission, especially in school settings,” said Brooke Nichols, an infectious disease modeler at the Boston University School of Public Health.
That is not to say that younger children do not become infected — they do. On Wednesday, Dr. Michael Beach, a senior scientist at the Centers for Disease Control and Prevention, acknowledged that the agency’s guidance on school reopenings does not reflect the latest research showing that children can become infected with the coronavirus and transmit it to others.
“It does appear that children can become infected” and that children “clearly can transmit,” Dr. Beach, the agency’s deputy incident manager for Covid-19 response, told the House Select Subcommittee on the Coronavirus Crisis.
… Weighed against the substantial harms to children and parents from keeping schools closed, elementary schools should at least offer in-person learning, said Dr. David Rubin, a pediatrician and infectious disease expert at the University of Pennsylvania.
How helpful is convalescent plasma, really? – BMJ
[editor’s note: A randomized trial in India found no benefit in slowing progression to severe COVID-19 or in all-cause mortality. This post was written in scientific style.]
Although the use of convalescent plasma seemed to improve resolution of shortness of breath and fatigue in patients with moderate covid-19 and led to higher negative conversion of SARS-CoV-2 RNA on day 7 post-enrolment, this did not translate into a reduction in 28 day mortality or progression to severe disease. Areas of future research could include effectiveness of convalescent plasma among neutralising antibody negative patients and the use of convalescent plasma with high neutralising antibody titres. The challenge will be to find both suitable patients and suitable plasma donors. Additionally, this challenge could limit the use of convalescent plasma to a small subset of patients.
Hospital Bills For Uninsured COVID-19 Patients Are Covered, But No One Tells Them – NPR
The CARES Act provides funds to pay medical bills for uninsured COVID-19 patients. But a young man’s death in Nashville, Tenn., shows people often don’t know about the program until it’s too late.
TriStar, like most major health systems, participates in a program through the Centers for Medicare and Medicaid Services in which uninsured patients with COVID-19 have their bills covered. It was set up through the pandemic relief legislation known as the CARES Act.
But TriStar doesn’t tell its patients that upfront. Neither do other hospitals or national health systems contacted by WPLN News. There’s no requirement to, which is one of the program’s shortcomings, says Jennifer Tolbert of the Kaiser Family Foundation who studies uninsured patients. (KHN is an editorially independent program of the foundation.)
“This is obviously a great concern to most uninsured patients,” Tolbert says. Her research finds that people without insurance often avoid care because of the bill or the threat of the bill, even though they might qualify for any number of programs if they asked enough questions.
Tolbert says the problem with the COVID-19 uninsured program is that even doctors don’t always know how it works or that the program exists.
COVID-19 Plus Cancer Proves Deadly – MedPage
Patients with cancer and COVID-19 have a higher risk of severe disease and mortality, researchers reported.
Of 89 cancer patients admitted to the intensive care unit (ICU) due to COVID-19, 32 died, a mortality rate of 36%, reported Michael Dang, MD, a critical care fellow at Memorial Sloan Kettering Cancer Center in New York City, at the virtual CHEST conference, the annual meeting of the American College of Chest Physicians.
… Mortality rates appeared to be higher among the patients with hematologic cancers, he said. Of the 51 patients with solid tumors, most commonly non-small cell lung cancer and breast cancer, 14 died, for a mortality rate of 27%; of the 38 patients with hematologic cancers, most commonly leukemia and lymphoma, 18 died, for a mortality rate of 47%.
Of the 59 patients requiring mechanical ventilation, 32 died, a 54% mortality rate. If the patient was neutropenic, the mortality was very high — six of nine died.
In the study, Dang and colleagues included critically ill patients who were being treated for cancer and COVID-19 from March 16 through June 30, 2020 in two ICUs. The patients had a mean age of 64, 58% were men, 66% were white, 18% were Black, and 10% were Asian/Indian. COVID-19 cases were confirmed via reverse-transcriptase polymerase chain reaction assays performed on nasopharyngeal swab specimens.
COVID Causes People to Lose Their Sense of Smell Because of Changes in the Brain, Study Suggests – Newsweek
The sudden loss of smell in some COVID-19 patients may be explained by changes to the brain, according to a study.
After the coronavirus that causes COVID-19 first emerged late last year, losing one’s sense of smell and taste quickly emerged as a possible symptoms of the disease. The U.S. Centers for Disease Control and Prevention lists these alongside other symptoms such as a fever or chills, cough, shortness of breath, and fatigue.
Study Co-author Maxime Niesen of the Functional Brain Mapping Laboratory at Belgium’s ULB university and colleagues set out to explore the hypothesis that some COVID-19 patients lose their sense of smell because the infection affects cells that support certain neurons that are key for this sense working.
It is also thought that inflammation stops certain receptors from picking up smells, and a person’s sense of smell is restored when this subsides, Professor Barry Smith, director of the Centre for the Study of the Senses at the U.K’s University of London who did not work on the paper, told Newsweek via email. If a person loses their sense of smell totally or partially for a longer period of time, this may be due to the overreaction of the immune system blocking receptors, he said.
After studying 12 COVID-19 patients, the authors of the paper suggested there are a number of reasons why they lost their sense of smell. Parts of the brain involved in processing smells, including what are known as the olfactory cleft, olfactory bulbs, and surrounding neural tissue were affected in some patients.
The team found that the infection appears to affect how parts of the brain involved in this sense metabolize sugar. And the connections of nerve cells that pass on information about smells may also be interrupted by the coronavirus infection.
The following are foreign headlines with hyperlinks to the posts
France’s Prime Minister Jean Castex grimly announced “the second wave is here” while implementing a new curfew.
India has reported below 60,000 new coronavirus cases for a fifth day as the promise of a free vaccine turned into a key state election issue.
Colombian pro cyclist Fernando Gaviria is confirmed to be among the emerging cases of re-infection — his second case asymptomatic after spending a month hospitalized last winter.
Poland limits gatherings, shutters bars and restaurants amid COVID-19 surge
COVID Cases Are Still Rising in These 80 Countries
Trump’s Harsh Sanctions on COVID-Stricken Iran Leave Diplomatic Wreckage
Lack of Antidotes Adds to Ethical Dilemmas for UK COVID-19 Challenge Trials
Nepal suspends access to Mount Everest after a local virus case is detected.
North Korea warns that dust storms from China may carry the virus.
Istanbul has 40 percent of Turkey’s virus cases, a top official reports.
Trudeau announces $214M for potential made-in-Canada COVID-19 vaccines
Uruguay will close its borders during summer season to prevent Covid-19 spread
‘It’s time for partying in nightclubs to stop’: Sweden limits clubs to 50 people
Russia records more than 17,000 cases for the first time
The following are additional national and state headlines with hyperlinks to the posts
Moments after hearing an Idaho hospital was overwhelmed by virus patients and looking at sending people as far away as Seattle
Social distancing in Major League Baseball, without the hard bubble used in pro basketball and hockey, was largely successful in mitigating COVID spread.
New England ice rinks shut down after coronavirus case clusters emerge linked to hockey
Researchers Find Doubts About COVID-19 Vaccine Among People Of Color
Trumps to host Halloween at White House despite coronavirus
COVID Outbreak At North Carolina Church Kills 3, Infects Nearly 100 People
California Gov. Newsom’s Thanksgiving Rules, Severe Restrictions in Place
Florida Will Investigate All COVID-19 Deaths
Britain Authorises Temporary Use of Flu Vaccine to Help Meet Demand
The U.S. reported its second-highest daily case total since the start of the pandemic.
One rural state continues to do a fabulous job keeping the virus away: Vermont.

West Point to Host Army-Navy Game for First Time Since World War II
More than 19,000 new Covid-19 cases recorded in Italy
Down syndrome tied to 10 times the risk of COVID-19 death
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
16 October 2020 ECRI’s WLI Marginally Continues To Improve
Rail Week Ending 17 October 2020 – Improvement Continues
A No-Deal Brexit Could Damage The UK’s Ability To Cope With Pandemics
Contact-tracing Apps: There’s No Evidence They’re Helping To Stop COVID-19
Warning to Readers
The amount of politically biased articles on the internet continues to increase. And studies and opinions of the experts continue to contradict other studies and expert opinions. Honestly, it is difficult to believe anything anymore. A study usually cannot establish cause and effect – but only correlation. Be very careful what you believe about this pandemic.

I assemble this coronavirus update daily – sifting through the posts on the internet. I try to avoid politically slanted posts (mostly from CNN, New York Times, and the Washington Post) and can usually find unslanted posts on that subject from other sources on the internet. I wait to publish posts on subjects that I cannot validate across several sources. But after all this extra work, I do not know if I have conveyed the REAL facts. It is my job to provide information so that you have the facts necessary – and then it is up to readers to draw conclusions.
Coronavirus INTERACTIVE Charts
include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus.htm’); ?>
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19. At this point, herd immunity does not look like an option although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a higher death rate.
- There are at least 8 strains of the coronavirus. New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
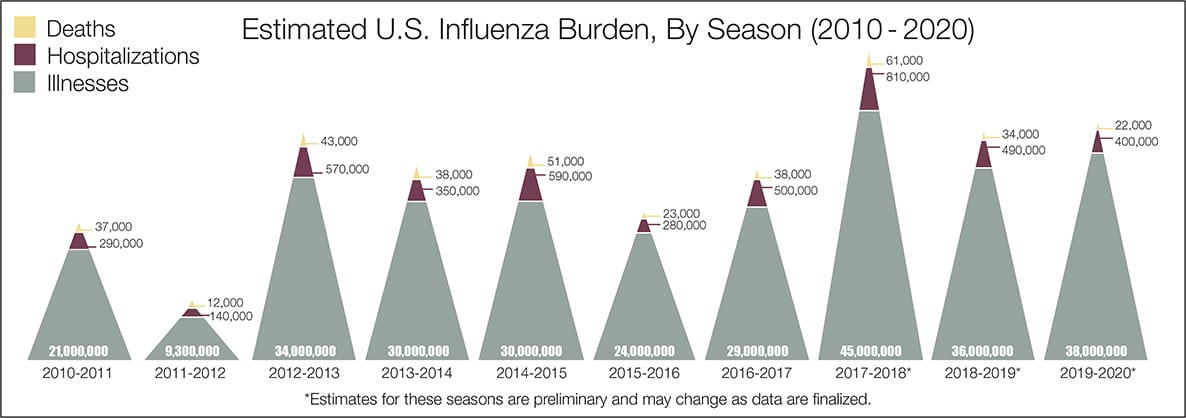
- The real question remains if the U.S. is over-reacting to this virus. The following graphic from the CDC puts the annual flu burden in perspective [click on image to enlarge]. Note that using this data is dangerous as the actual flu cases are estimated and not counted – nobody knows how accurate these guesses are.
What we do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work.
- Do we develop lasting immunity to the coronavirus? Another coronavirus – the simple cold – does not develop long term immunity.
- To what degree do people who never develop symptoms contribute to transmission?
- The US has scaled up coronavirus testing – and the accuracy of the tests has been improving. However, if one loses immunity – the coronavirus testing value is reduced.
- Can children widely spread coronavirus? [current thinking is that they are becoming a major source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- What effect will the weather have? At this point, it does not seem hot weather slows this coronavirus down – and it seems air conditioning contributes to its spread.
- Outdoor activities seem to be a lower risk than indoor activities.
- Can the world really push out an effective vaccine in 12 to 18 months?
- Will other medical treatments for Covid-19 ease symptoms and reduce deaths? So far only one drug (remdesivir) is approved for treatment.
- A current scientific understanding of the way the coronavirus works can be found [here].
Heavy breakouts of coronavirus have hit farm workers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of the respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
Human coronaviruses ‘inactivated’ by mouthwash, oral rinses
| New coronavirus restrictions in Chicago go into effect Friday for two weeks as the nation’s third largest city fights a surge of COVID-19 infections. Mayor Lori Lightfoot announced a 10 p.m. curfew for all nonessential businesses and ordered bars and breweries without food licenses to shut down indoor service. |
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>





