Written by Steven Hansen
The U.S. new cases 7-day rolling average is 15.6 % HIGHER than the 7-day rolling average one week ago. U.S. deaths due to coronavirus are now 4.5 % LOWER than the rolling average one week ago. At the end of this post is a set of interactive graphs and tables for the world and individual States – as well as today’s headlines which include;
- WHO (Accidentally) Confirms Covid is No More Dangerous Than Flu
- Johnson & Johnson Temporarily Pauses All Dosing in Its COVID-19 Vaccine Trials
- 20% excess deaths over expected deaths between March 1 and August 1 – of which 67% attributed to COVID-19
- Drug RLF-100 (aviptadil) increased the likelihood of COVID survival
- Multiple coronavirus vaccines should be available by spring, but learning which is most effective will likely come later.
- A vaccine can provide better immunity than an actual infection
- White House Appears to Endorse Herd Immunity Strategy for COVID-19
- COVID-19 Antibodies Last at Least 3 Months
- Rising COVID-19 Cases Could Indicate Next Surge
- Dr. Fauci Says U.S. is ‘Facing A Whole Lot of Trouble’ With Coronavirus Cases as Temperatures Drop

The recent worsening of the trendlines for new cases should be attributed to going back to school (especially at college/university level) and continued loosening of regulations designed to slow the coronavirus spread.
My continuing advice is to continue to wash your hands, wear masks, and maintain social distancing. No handwashing, mask, or social distancing will guarantee you do not get infected – but it sure as hell lowers the risk in all situations – and evidence to-date shows a lower severity of COVID-19. In addition, certain activities are believed to carry a higher risk – like being inside in air conditioning and removing your mask (such as restaurants, around your children/grandchildren, bars, and gyms). It is all about viral load – and outdoor activities are generally very safe.
The daily number of new cases in the U.S. is remaining stubbornly and embarrassedly high.
The following graphs show the 7-day rolling average for new coronavirus cases and deaths have been updated through 13 October 2020:


z coronavirus.png
Coronavirus Statistics For 13 October 2020 |
| U.S. Only | Global | U.S Percentage of Total | ||||
| Today*** | Cumulative | Today*** | Cumulative | Today | Cumulative | |
| New Confirmed Cases | 49,378 | 7,800,000 | 332,764 | 37,880,000 | 14.8% | 20.6% |
| Deaths** | 314 | 215,085 | 3,912 | 1,080,000 | 8.0% | 19.9% |
| Mortality Rate | 0.6% | 2.8% | 1.2% | 2.9% | ||
total COVID-19 Tests per 1,000 people | 2.11* | 367.35* | ||||
Source: EU CDC
* as of 05 Oct 2020
** evidently several States included “probable” deaths today in the number
*** red color indicates record number
Europe and Asia are now doing worse than the U.S. in the race to see who can have more new cases.

Coronavirus News You May Have Missed
WHO (Accidentally) Confirms Covid is No More Dangerous Than Flu – Off-Guardian
Head of Health Emergencies Program “best estimates” put IFR at 0.14%
The World Health Organization has finally confirmed what we (and many experts and studies) have been saying for months – the coronavirus is no more deadly or dangerous than seasonal flu.
The WHO’s top brass made this announcement during a special session of the WHO’s 34-member executive board on Monday October 5th, it’s just nobody seemed to really understand it.
In fact, they didn’t seem to completely understand it themselves.
At the session, Dr Michael Ryan, the WHO’s Head of Emergencies revealed that they believe roughly 10% of the world has been infected with Sars-Cov-2. This is their “best estimate”, and a huge increase over the number of officially recognised cases (around 35 million).
Dr. Margaret Harris, a WHO spokeswoman, later confirmed the figure, stating it was based on the average results of all the broad seroprevalence studies done around the world.
As much as the WHO were attempting to spin this as a bad thing – Dr Ryan even said it means “the vast majority of the world remains at risk.” – it’s actually good news. And confirms, once more, that the virus is nothing like as deadly as everyone predicted.
Johnson & Johnson Temporarily Pauses All Dosing in Our Janssen COVID-19 Vaccine Candidate Clinical Trials – Johnson & Johnson
We have temporarily paused further dosing in all our COVID-19 vaccine candidate clinical trials, including the Phase 3 ENSEMBLE trial, due to an unexplained illness in a study participant. Following our guidelines, the participant’s illness is being reviewed and evaluated by the ENSEMBLE independent Data Safety Monitoring Board (DSMB) as well as our internal clinical and safety physicians.
Adverse events – illnesses, accidents, etc. – even those that are serious, are an expected part of any clinical study, especially large studies. Based on our strong commitment to safety, all clinical studies conducted by the Janssen Pharmaceutical Companies of Johnson & Johnson have prespecified guidelines. These ensure our studies may be paused if an unexpected serious adverse event (SAE) that might be related to a vaccine or study drug is reported, so there can be a careful review of all of the medical information before deciding whether to restart the study.
We must respect this participant’s privacy. We’re also learning more about this participant’s illness, and it’s important to have all the facts before we share additional information.
Excess Deaths From COVID-19 and Other Causes, March-July 2020 – JAMA
Between March 1 and August 1, 2020, 1 336 561 deaths occurred in the US, a 20% increase over expected deaths (1 111 031 [95% CI, 1 110 364 to 1 111 697]). The 10 states with the highest per capita rate of excess deaths were New York, New Jersey, Massachusetts, Louisiana, Arizona, Mississippi, Maryland, Delaware, Rhode Island, and Michigan. The states with the highest per capita rate of excess deaths changed from week to week (Video). The increase in absolute deaths in these states relative to expected values ranged from 22% in Rhode Island and Michigan to 65% in New York (Table). Three states with the highest death rates (New Jersey, New York, and Massachusetts) accounted for 30% of US excess deaths but had the shortest epidemics (ED90 < 10 weeks). States that experienced acute surges in April (and reopened later) had shorter epidemics that returned to baseline in May, whereas states that reopened earlier experienced more protracted increases in excess deaths that extended into the summer (Figure).
Of the 225 530 excess deaths, 150 541 (67%) were attributed to COVID-19. Joinpoint analyses revealed an increase in deaths attributed to causes other than COVID-19, with 2 reaching statistical significance. US mortality rates for heart disease increased between weeks ending March 21 and April 11 (APC, 5.1 [95% CI, 0.2-10.2]), driven by the spring surge in COVID-19 cases. Mortality rates for Alzheimer disease/dementia increased twice, between weeks ending March 21 and April 11 (APC, 7.3 [95% CI, 2.9-11.8]) and between weeks ending June 6 and July 25 (APC, 1.5 [95% CI, 0.8-2.3]), the latter coinciding with the summer surge in sunbelt states.
Although total US death counts are remarkably consistent from year to year, US deaths increased by 20% during March-July 2020. COVID-19 was a documented cause of only 67% of these excess deaths. Some states had greater difficulty than others in containing community spread, causing protracted elevations in excess deaths that extended into the summer. US deaths attributed to some noninfectious causes increased during COVID-19 surges. Excess deaths attributed to causes other than COVID-19 could reflect deaths from unrecognized or undocumented infection with severe acute respiratory syndrome coronavirus 2 or deaths among uninfected patients resulting from disruptions produced by the pandemic. Study limitations include the reliance on provisional data, inaccuracies in death certificates, and assumptions applied to the model.
Amid Regeneron’s emergency use bid, former FDA chief says U.S. ‘too late’ on mass manufacture of COVID-19 antibodies – Fierce Pharma
Days removed from its star turn in President Donald Trump’s COVID-19 treatment, Regeneron’s antibody cocktail could be on the fast track to an emergency approval. But if it gets there, will there be enough supply to meet this year’s demand? That boat’s already sailed, a former FDA chief warned.
As Regeneron pursues an emergency use authorization for the cocktail, drugmakers are already “too late” scaling up manufacturing to produce enough antibody doses to meet demand this year, former FDA Commissioner Scott Gottlieb, M.D., said Sunday.
On CBS’ Face the Nation, Gottlieb forecast the U.S. would need to produce between 300,000 and 400,000 antibody treatment courses each month to keep up with continued demand in what he called a potentially “difficult fall and winter.”
In an earlier segment on the show, Regeneron CEO Len Schleifer noted the company only has around 50,000 treatment courses stocked but is working toward supplying 300,000 courses to the U.S. within the next few months as part of a $450 million contract signed in July.
“We would have needed to take different steps in April and May to ramp up manufacturing capacity to have the drug available in larger quantities now,” Gottlieb said. “It’s too late for this year. I think we could still take steps to do it for 2021, but we’re stuck with the doses we have.”
Relief Therapeutics said its investigational drug RLF-100 (aviptadil) increased the likelihood of survival – NwueoRX
RELIEF THERAPEUTICS Holding AG (SIX: RLF, OTCQB: RLFTF) (“Relief” or the “Company“) and NeuroRx, Inc., today announced topline results from 45 patients assessed in an open-label prospective study where 21 patients admitted to an intensive care unit (ICU) with critical COVID-19 and respiratory failure were treated with RLF-100™(aviptadil) and compared to 24 control patients treated in the same setting. All patients had severe comorbidities that rendered them ineligible for the ongoing randomized, controlled phase 2b/3 trial being conducted to ascertain safety and efficacy of RLF-100™, and all patients were deteriorating despite treatment with approved therapies for COVID-19.
Overall, 81% of RLF-100™-treated patients survived beyond 60 days, compared to 17% of control patients. Patients treated with RLF-100™ demonstrated a 9-fold increased probability of survival and recovery from respiratory failure, with a high degree of statistical significance. Statistical analysis was performed by Prof. Phil Lavin, FASA, FRAPS of the Boston Biostatistical Research Foundation.
“We are encouraged by these initial results in highly comorbid patients with COVID-19 respiratory failure, and we are pleased that the majority of these patients have returned safely to their families. We look forward to the upcoming results from the randomized, double-blind, prospective trial in less severely comorbid patients for confirmation of these results,” said Jihad Georges Youssef, MD, section chief of General Academic Pulmonary Medicine at the Houston Methodist Hospital, who serves as the study’s principal investigator at Houston Methodist and also serves as national co-chair for the ongoing randomized controlled trial.
“The patients included in this study are representative of those who are too ill to be included in the clinical trials of any known treatment for COVID-19,” said Dr. Jonathan Javitt, CEO and Chairman of NeuroRx, Inc. “We are grateful to Dr. Youssef and to the Houston Methodist Hospital for having the courage to treat and study patients at this level of risk. The results suggest that there may be substantial hope to mitigate the attack of the coronavirus on the delicate cells that line the lung with a natural peptide that has been protecting the lung’s lining since humans first walked the earth. While the number of patients treated at Houston Methodist is modest, the initial results in our nationwide expanded access program suggest similarly encouraging survival with RLF-100™. We continue to closely monitor treatment with RLT-100TM in other hospitals.”
ABBOTT RECEIVES FDA EMERGENCY USE AUTHORIZATION FOR ITS COVID-19 IGM ANTIBODY BLOOD TEST – Abbott
Abbott (NYSE: ABT) announced today that the U.S. Food and Drug Administration (FDA) issued Emergency Use Authorization (EUA) for the company’s AdviseDx SARS-CoV-2 IgM (Immunoglobulin M) lab-based serology test for use on the ARCHITECT® and Alinity™ platforms. IgM antibody testing can play an important role in understanding if someone has developed antibodies in response to the virus, indicating a recent or prior infection.
The new IgM antibody test is Abbott’s latest test to support in the fight against COVID-19. Since the start of the pandemic, Abbott has received emergency use authorization for seven tests, including molecular tests, a rapid antigen test and an IgG antibody test.
“Abbott has developed tests to detect the virus at each stage of infection so doctors and their patients are equipped with knowledge of how they are responding to the virus and progressing through recovery,” said Robert B. Ford, president and chief executive officer, Abbott. “Antibody tests will continue to play an important role to better understand the virus, the prevalence of COVID-19 in an area and where a patient may be in their recovery.”
Multiple coronavirus vaccines should be available by spring, but learning which is most effective will likely come later. – New York Times
… The first vaccines may provide only moderate protection, low enough to make it prudent to keep wearing a mask. By next spring or summer, there may be several of these so-so vaccines, without a clear sense of how to choose from among them. Because of this array of options, makers of a superior vaccine in early stages of development may struggle to finish clinical testing. And some vaccines may be abruptly withdrawn from the market because they turn out not to be safe.
“It has not yet dawned on hardly anybody the amount of complexity and chaos and confusion that will happen in a few short months,” said Dr. Gregory Poland, the director of the Vaccine Research Group at the Mayo Clinic.
Some of this confusion is inevitable, but some is the result of how coronavirus vaccine trials were designed: Each company is running its own trial, comparing its jab with a placebo. But it didn’t have to be this way.
… But the efficacy in a trial may not necessarily match its effectiveness out in the real world. That’s because, like any statistical study, Phase 3 trials have margins of error. A vaccine that met the F.D.A.’s guidelines might actually be more than 50 percent effective, or might be less so. It might well turn out to be only 35 percent effective.
… Things could be even worse for vaccines in earlier stages of testing. Those products might have to prove that they are better than the newly approved vaccine. The difference between two vaccines will be smaller than between a vaccine and a placebo. As a result, these trials may have to be bigger and run longer. The steep cost may be more than many of the small start-ups working on innovative vaccines can afford.
“That basically prevents the development of better vaccines,” said Dr. Naor Bar-Zeev, a vaccine expert at the Johns Hopkins University School of Medicine. “Given the massive taxpayer investment, the public should demand better.”
[editor’s note: this post confirms what I have been saying – the real study occurs after the vaccine is given to the general population]
A vaccine can provide better immunity than an actual infection. – CNN
Two recent studies have confirmed that two people previously infected with SARS-CoV-2, the virus that causes Covid-19, can be reinfected with the virus.
Interestingly, the two people had different outcomes. The person in Hong Kong showed no symptoms on the second infection, while the person from Reno, Nevada, had a more severe version of the disease the second time around. It is therefore unclear if an immune response to SARS-CoV-2 will protect against subsequent reinfection.
Does this mean a vaccine will also fail to protect against the virus? Certainly not. First, it is still unclear how common these reinfections are. More importantly, a fading immune response to natural infection, as seen in the Nevada patient, does not mean we cannot develop a successful, protective vaccine.
… Vaccines have other advantages over natural infections. For one, they can be designed to focus the immune system against specific antigens that elicit better responses.
For instance, the human papillomavirus (HPV) vaccine elicits a stronger immune response than infection by the virus itself. One reason for this is that the vaccine contains high concentrations of a viral coat protein, more than what would occur in a natural infection. This triggers strongly neutralizing antibodies, making the vaccine very effective at preventing infection.
The natural immunity against HPV is especially weak, as the virus uses various tactics to evade the host immune system. Many viruses, including HPV, have proteins that block the immune response or simply lie low to avoid detection. Indeed, a vaccine that provides accessible antigens in the absence of these other proteins may allow us to control the response in a way that a natural infection does not.
[editor’s note: hard to summarize this post – deserves a full read]
White House Appears to Endorse Herd Immunity Strategy for COVID-19 – MedPage
The Trump administration Monday appeared to endorse a strategy of herd immunity for the COVID-19 pandemic without waiting for vaccines to be rolled out, with one White House official saying that “we cannot eliminate all cases, so what we do is focus on saving lives.”
Two administration officials held a press call — speaking on condition of anonymity — to discuss the Great Barrington Declaration, which was issued on Oct. 4. The declaration states,”Current lockdown policies are producing devastating effects on short and long-term public health,” and argues that keeping lockdown measures in place “until a vaccine is available will cause irreparable damage, with the underprivileged disproportionately harmed.”
However, the officials didn’t indicate when a formal policy would be issued or what it would look like; the federal government’s ability to overrule public health measures taken by the states and local governments is severely limited.
In fact, the unusual format for announcing the shift in policy — not offered as a prelude to an executive order or presidential address, as is typical for White House “backgrounders” — may suggest the press call was merely a trial balloon to gauge public response.
“The most compassionate approach that balances the risks and benefits of reaching herd immunity, is to allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk,” the declaration says. It also argues that while vaccines can “assist” in developing herd immunity, society should not depend on them.
[editor’s note: there is a certain element of herd immunity in even believing immunization will knock down the coronavirus. I am skeptical that the vaccines in trial will be able to make a huge enough dent in new cases – I hope I am wrong. Therefore, we must take many paths to defeat this virus.]
COVID-19 Antibodies Last at Least 3 Months – Reuters
People infected with COVID-19 develop antibodies targeting the new coronavirus that last for at least three months, according to two reports in Science Immunology.
The two studies, together involving nearly 750 patients, both point to immunoglobulin G (IgG) antibodies as the longest-lasting.
Researchers found IgG antibodies with two targets – the spike protein on the virus that helps it infect cells, and a part of the spike called the receptor binding domain (RBD) – lasted more than 100 days.
While the protective effect of COVID-19 antibodies is not completely clear, Jen Gommerman of the University of Toronto, coauthor of the study, said her team also found levels of so-called neutralizing antibodies, which inactivate the virus, “appeared to be very stable.”
The other study, from Harvard Medical School, reported similar findings.
This means that a properly designed vaccine “should elicit a durable antibody response that has the potential to neutralize the virus,” Gommerman said.
Rising COVID-19 Cases Could Indicate Next Surge – Medscape
A renewed increase in coronavirus cases and hospitalizations across the country could mean the predicted fall surge in COVID-19 has arrived, according to CNN.
In early September, the U.S. reported its lowest numbers at around 30,000-35,000 new cases per day. Now the numbers are back up around 45,000-50,000 new daily cases.
That increase will likely continue, Pater Hotez, MD, dean of the Baylor College of Medicine’s National School of Tropical Medicine, told CNN.
“This is the fall/winter surge that everyone was worried about. And now it’s happening,” he said. “And it’s happening especially in the northern Midwest, and the Northern states are getting hit very hard — Wisconsin, Montana, the Dakotas. But it’s going to be nationally soon enough.”
During the past week, 33 states reported more coronavirus cases than the previous week, and 10 states have reported record-high hospitalizations since Friday, the news outlet reported. In Denver, the latest case counts are as high as they were back in May. In Wisconsin, public health officials reported a record-high of COVID-19 cases, hospitalizations and deaths last week.
“This winter — this November, December, January, February — could be the worst time in our epidemic,” Hotez said. “Get ready to hunker down.”
Dr. Fauci Says U.S. is ‘Facing A Whole Lot of Trouble’ With Coronavirus Cases as Temperatures Drop – Newsweek
Dr. Anthony Fauci warned Monday that the U.S. could face an increase in positive cases of COVID-19 as the weather becomes cooler.
Recent data indicated more than 8 million U.S. cases of coronavirus, with 220,010 deaths attributable to the virus. Some states are seeing a surge in positive cases, spreading resources thin. President Donald Trump, who contracted the virus in early October, said during a Saturday address that the virus would soon “disappear.”
In a Monday interview with Shephard Smith on CNBC, Fauci said he believed that the U.S. is “facing a whole lot of trouble.”
“We have a baseline of infections now that vary between 40,000 and 50,000 per day,” Fauci said. “That’s a bad place to be when you’re going into the cooler weather of the fall and the colder weather of the winter.”
Fauci explained that the combination of a higher baseline number of positive cases combined with chilly temperatures could make more people stay indoors. Fauci called that situation “a perfect set-up for an acceleration of respiratory-borne diseases.”
“We’re in a bad place now,” Fauci added. “We’ve gotta turn this around.”
The following are foreign headlines with hyperlinks to the posts
England is currently reporting more hospitalized COVID-19 patients than in March, and areas with high numbers of infections will face new restrictions.
Meanwhile in France, ICUs are at their highest capacity since late May.
IMF upgrades economic forecast but warns of long-term coronavirus damage
Russia Breaks New Coronavirus Cases Record for Third Time in a Week
Soccer Legend Cristiano Ronaldo Tests Positive For COVID-19
COVID Vaccine Update, France’s Sanofi Aims for Mid-2021 Rollout
First COVID Reinfection Death Recorded in Netherlands
Iceland’s tourism industry is preparing for a comeback.
Iran’s coronavirus daily death tolls hit record highs as currency falls to historic low
Protests as Argentina’s cases pass 900,000
A “second wave” of mental health devastation due to Covid-19 is imminent, experts say
The following are additional national and state headlines with hyperlinks to the posts
We’re public health experts. We need to do a better job of talking to conservatives.
Scientists Confirm Nevada Man Was Infected Twice With Coronavirus
Regeneron officials sell $1M in stock after Trump calls COVID-19 treatment drugs ‘miracles’
New York Philharmonic Cancels Its Entire 2020-21 Season, Due To Coronavirus
Wisconsin Judge Upholds Governor’s Statewide Mask Mandate
Florida governor doesn’t wear mask to Trump rally
COVID-19: A Second Wave of Mental Illness ‘Imminent’
Pew: COVID Sends Majority of Young Adults Back Home
COVID-19 Symptoms Linger for Months for Many
Perforated Appendicitis in Kids More Common After COVID-19 Outbreak
Oklahoma City Runs out of ICU Beds as COVID Cases Spike
Half of the 20 Metro Areas Worst-Hit by COVID Are All in One State
Only 44 Coronavirus Cases Documented Among 1 Billion Air Travelers in 2020
Number of Americans Who Say They’d Get a COVID-19 Vaccine Hits Record Low
Autopsies Show Coronavirus in the Eyeballs of Victims
July is the new January: More companies delay a return to the office.
18 employees at Las Vegas USPS facility test positive for COVID-19
Facebook says it will ban anti-vaccination ads
U.S. Army chief returns to Pentagon after self-quarantine
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
September 2020 Consumers’ Spending Expectations Improve
September 2020 CPI: Year-over-Year Inflation Rate Marginally Grows to 1.4%
July 2020 Loan Performance: Late-Stage Delinquencies Spiked To Highest Level Since 1999
September 2020 Small Business Optimism Improves, Uncertainty Index Remains High
Should Emerging Economies Embrace Quantitative Easing During The Pandemic?
Post-COVID Recovery? Not So Fast, My Friend
A Radical Nature-Based Agenda Would Help Society Overcome The Psychological Effects Of Coronavirus
More Stimulus And The 2nd Derivative Effect
Being Outdoors Doesn’t Mean You’re Safe From COVID-19 A White House Event Showed What Not To Do
Warning to Readers
The amount of politically biased articles on the internet continues to increase. And studies and opinions of the experts continue to contradict other studies and expert opinions. Honestly, it is difficult to believe anything anymore. A study usually cannot establish cause and effect – but only correlation. Be very careful what you believe about this pandemic.

I assemble this coronavirus update daily – sifting through the posts on the internet. I try to avoid politically slanted posts (mostly from CNN, New York Times, and the Washington Post) and can usually find unslanted posts on that subject from other sources on the internet. I wait to publish posts on subjects that I cannot validate across several sources. But after all this extra work, I do not know if I have conveyed the REAL facts. It is my job to provide information so that you have the facts necessary – and then it is up to readers to draw conclusions.
Coronavirus INTERACTIVE Charts
include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus.htm’); ?>
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19. At this point, herd immunity does not look like an option although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a higher death rate.
- There are at least 8 strains of the coronavirus. New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
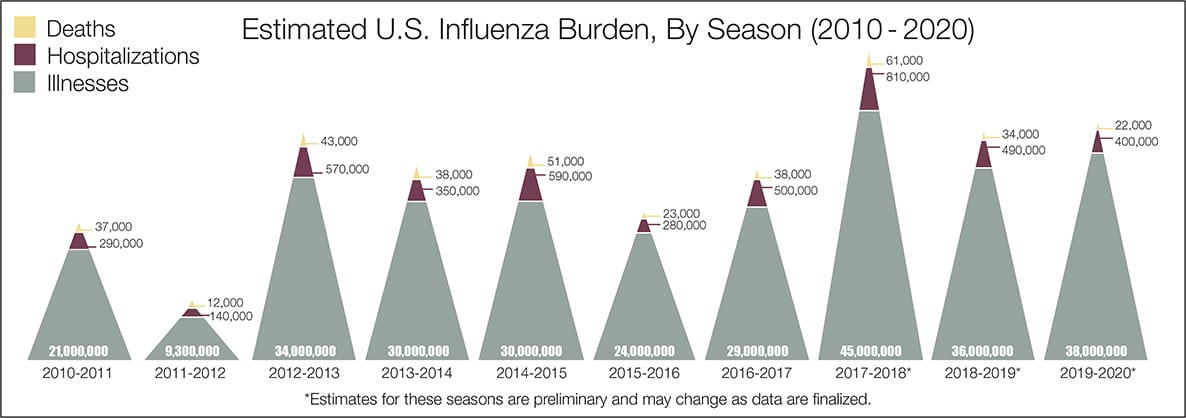
- The real question remains if the U.S. is over-reacting to this virus. The following graphic from the CDC puts the annual flu burden in perspective [click on image to enlarge]. Note that using this data is dangerous as the actual flu cases are estimated and not counted – nobody knows how accurate these guesses are.
What we do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work.
- Do we develop lasting immunity to the coronavirus? Another coronavirus – the simple cold – does not develop long term immunity.
- To what degree do people who never develop symptoms contribute to transmission?
- The US has scaled up coronavirus testing – and the accuracy of the tests has been improving. However, if one loses immunity – the coronavirus testing value is reduced.
- Can children widely spread coronavirus? [current thinking is that they are becoming a major source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- What effect will the weather have? At this point, it does not seem hot weather slows this coronavirus down – and it seems air conditioning contributes to its spread.
- Outdoor activities seem to be a lower risk than indoor activities.
- Can the world really push out an effective vaccine in 12 to 18 months?
- Will other medical treatments for Covid-19 ease symptoms and reduce deaths? So far only one drug (remdesivir) is approved for treatment.
- A current scientific understanding of the way the coronavirus works can be found [here].
Heavy breakouts of coronavirus have hit farm workers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of the respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>





