Written by Steven Hansen
The U.S. new cases 7-day rolling average is 2.1 % LOWER than the 7-day rolling average one week ago. U.S. deaths due to coronavirus are now 3.9 % LOWER than the rolling average one week ago. At the end of this post is a set of interactive graphs and tables for the world and individual States – as well as today’s headlines which include;
- New Global Lab Network Will Compare COVID-19 Vaccines Head-to-Head
- US Schools in Suburbs, Small Cities Reopening Without COVID Spike; Big Cities Up Next
- Trump doctors clear discharge, but not “out of the woods yet”
- Use of Regeneron’s experimental coronavirus treatment for President Trump creates ‘very tough situation,’
- Inside the Flawed White House Testing Scheme That Did Not Protect Trump
- A new culprit for severe COVID-19 cases

The recent worsening of the trendlines for new cases should be attributed to going back to school (especially at college/university level) and continued loosening of regulations designed to slow the coronavirus spread.
My continuing advice is to continue to wash your hands, wear masks, and maintain social distancing. No handwashing, mask, or social distancing will guarantee you do not get infected – but it sure as hell lowers the risk in all situations – and evidence to-date shows a lower severity of COVID-19. In addition, certain activities are believed to carry a higher risk – like being inside in air conditioning and removing your mask (such as restaurants, around your children/grandchildren, bars, and gyms). It is all about viral load – and outdoor activities are generally very safe.
The daily number of new cases in the U.S. is remaining stubbornly and embarrassedly high.
The following graphs show the 7-day rolling average for new coronavirus cases and deaths have been updated through 05 October 2020:


z coronavirus.png
Coronavirus Statistics For 05 October 2020 |
| U.S. Only | Global | U.S Percentage of Total | ||||
| Today*** | Cumulative | Today*** | Cumulative | Today | Cumulative | |
| New Confirmed Cases | 43,257 | 7,420,000 | 292,021 | 35,250,000 | 14.8% | 21.0% |
| Deaths** | 400 | 209,794 | 3,814 | 1,040,000 | 10.5% | 20.2% |
| Mortality Rate | 0.9% | 2.8% | 1.3% | 3.0% | ||
total COVID-19 Tests per 1,000 people | 1.98* | 357.13* | ||||
* as of 02 Oct 2020
** evidently several States included “probable” deaths today in the number
*** red color indicates record number
Coronavirus News You May Have Missed
Trump doctors clear discharge, but not “out of the woods yet” – CBS
The medical team treating President Trump for COVID-19 at Walter Reed National Military Medical Center said he has improved enough to return to the White House on Monday, but warned he is not yet fully in the clear and declined to provide key details about the president’s condition.
“Though he may not entirely be out of the woods yet, the team and I agree that all our evaluations, and more importantly, his clinical status, support the president’s safe return home, where he’ll be surrounded by world-class medical care, 24/7,” Dr. Sean Conley, the White House physician, told reporters outside the facility on Monday afternoon.
Mr. Trump continues to be treated with dexamethasone, a powerful steroid recommended for use to treat severe cases of COVID-19 that can carry serious psychological side effects. Conley said the president has not exhibited any of those side effects. He repeatedly declined to provide specifics about the president’s lung condition and the last time he tested negative for the virus, citing federal privacy laws.
… At the briefing outside Walter Reed, Conley and the rest of the president’s medical team said Mr. Trump has “continued to improve” and “met or exceeded all standard hospital discharge criteria,” allowing him to return to the White House after just three days in the hospital.
“We try to get patients out of the hospital as quickly as it is safe and reasonable,” Conley said. “Every day that a patient stays in the hospital unnecessarily is a risk to themselves.”
The doctors said the president was not complaining of any respiratory issues and last had a fever more than 72 hours ago. Mr. Trump will receive the fourth of five doses of the drug remdesivir before leaving Walter Reed later Monday, and continues to be treated with dexamethasone, a steroid.
“We send patients home with medicines all the time,” Conley said. “He’s returning to a facility, the White House medical unit, that’s staffed 24/7, top-notch physicians, nurses, PAs, logisticians.”
Conley faced repeated questions about the safety of discharging the president to the White House when he remains infectious, as well as the decision to allow him to ride in an SUV to wave to supporters on Sunday. Conley said those around the president have taken the necessary precautions to avoid contracting the virus.
“The president has been surrounded by medical and security staff for days, wearing full PPE,” he said. “Yesterday the U.S. Secret Service agents were in the same level of PPE for a very short period of time.”
Conley declined to answer questions about the president’s lung scans and testing history, citing federal privacy laws. He added that the possibility of returning to the campaign trail remains uncertain.
“The big first thing that we need to do is [see] that there is no evidence of live virus still present that he could possibly transmit to others,” he said.
New Global Lab Network Will Compare COVID-19 Vaccines Head-to-Head – Pharmacist
The nonprofit Coalition for Epidemic Preparedness Innovations (CEPI) has created an international network of laboratories involved in conducting trials of COVID-19 vaccine candidates. The goal is to allow scientists and drugmakers to compare the potential vaccines and accelerate selection of the most effective candidates. The network encompasses labs in Europe, Asia, and North America, and will centralize the evaluation of samples “as though vaccines are all being tested under one roof” to curb the risk of variation in results, explains Melanie Saville, CEPI’s director of vaccine R&D. She notes when “everyone develops their own assays, they all use different protocols and different reagents—so while you get a readout, the ability to compare between different candidates is very difficult.” CEPI’s network will initially involve six labs from Canada, Britain, Italy, the Netherlands, Bangladesh, and India, Saville says. CEPI says all developers of potential COVID-19 vaccines can use its lab network at no cost to analyze their candidates against a common protocol. The network is initially assessing samples from early-stage vaccine candidate testing as well as Phase I and II human trials, but CEPI said it hoped to expand its capacity to Phase III trial data in the coming months. Neither CEPI nor the network will own the data, and results produced by the network will be sent back to the developer. CEPI itself is co-funding nine potential COVID-19 vaccines, including candidates from Moderna, AstraZeneca, Novavax, and CureVac.
The C.D.C. cites new evidence that the virus can spread beyond six feet indoors. – New York Times
Two weeks after the Centers for Disease Control and Prevention removed online guidance about airborne transmission of the coronavirus, the agency has replaced it with language citing new evidence that the virus can spread beyond six feet indoors, adrift in the air.
“These transmissions occurred within enclosed spaces that had inadequate ventilation,” the new guidance said. “Sometimes the infected person was breathing heavily, for example while singing or exercising.”
Notably, the new version is missing a previous statement that said the virus can be “airborne,” a term that would require hospitals to treat infected patients in specialized rooms and health care workers to wear N95 masks anywhere in a hospital.
The new version says the virus can be spread by both larger droplets and smaller aerosols released when people “cough, sneeze, sing, talk, or breathe.” But while the virus can be airborne under some circumstances, this is not the primary way the virus spreads.
Woman With COVID Shed Virus for 61 Days in Longest Case of Its Kind Recorded – Newsweek
A woman with COVID-19 who had a normal immune response to the infection was found to have shed the virus for 61 days. This is the longest known period of viral shedding in an immunocompetent patient, raising questions about how long patients may be contagious for, and the implications for those who are infected for prolonged periods.
Research suggests that the amount of time a person with SARS-CoV-2 will be infectious varies widely and is, to an extent, dependent on how severe their illness is. One way to identify this is based on “viral shedding.”
This is where the virus is replicating inside the body and being released into the environment. People with severe cases tend to shed the virus for longer, particularly in those who are immunocompromised or immunodeficient—either as a result of illness or therapy.
… The case report, published in the BMJ, identifies a 78-year-old woman who was hospitalized for breathlessness and discharge coming from her tracheostomy site. After being admitted, she tested positive for SARS-CoV-2. She continued to test positive for 61 days
Over the course of her hospitalization, she was treated with antibiotics but had no experimental or trial therapies. Physicians treating her wore personal protective equipment (PPE) and she was isolated throughout.
Trump Gets Experimental COVID Tx – Medpage
… An earlier statement from White House physician Sean Conley, DO, said the president had received “a single 8 gram dose of Regeneron’s polyclonal antibody cocktail,” which was completed “without incident.”
Regeneron had released topline results for its investigational REGN-COV2 antibody cocktail on Tuesday: the phase I/II/III trial showed the drug “reduced viral load and the time to alleviate symptoms in non-hospitalized patients with COVID-19,” as well as showing positive trends towards reducing medical visits.
But the product has not received FDA approval emergency use authorization yet, making it truly investigational. Some physicians on Twitter were puzzled that the president was using it. Jeremy Faust, MD, of Brigham and Women’s Hospital in Boston, tweeted that the president’s team either “can’t read basic medical literature” or “can read basic medical literature, but can’t overrule what [the president] is telling them to do” — or the president’s condition is far more serious than reported, and they are trying everything.
- The president, who announced Friday that he tested positive for the coronavirus, was given an 8 gram dose of Regeneron’s monoclonal antibody treatment, his doctors said.
- The company said it provided the drug to the president in response to a “compassionate use” request from Trump’s doctors.
- That means that while the president’s doctors were confident enough of the drug’s benefit to administer it to Trump, the treatment remains unavailable to most Americans.
Infected Trump greets supporters in motorcade outside hospital – Reuters
Trump, 74, wore a mask as he waved from the back seat of a black SUV that crawled in a caravan of vehicles in front of the Walter Reed National Military Medical Center outside Washington, while supporters waving Trump 2020 flags chanted: “USA! USA!”
Trump, who said on Friday morning he had the infectious disease, was swiftly criticized for risking the health of support staff.
It was Trump’s first appearance in public since he was evacuated to the hospital on Friday.
“It’s a very interesting journey. I learned a lot about COVID,” he said in a video posted on Twitter shortly beforehand.
… Critics said personnel who traveled in Trump’s armored SUV during the afternoon motorcade would now have to self-quarantine for 14 days. “The irresponsibility is astounding,” Dr. James Phillips, an attending physician at the hospital, said on Twitter.
The White House Correspondents Association objected that reporters had not been told about Trump’s drive-by before it happened.
White House spokesman Judd Deere said the trip had been approved by medical staff and that appropriate precautions had been taken.
Prospect of Trump’s early hospital discharge mystifies doctors – Washington Post
The assertion by President Trump’s doctors that he could be discharged from the hospital as early as Monday astonished outside infectious-disease experts, who said he remains in a dangerous period of vulnerability when some covid-19 patients decline precipitously and require urgent intervention.
“My impression is they are telling us everything that is of good news and limiting everything that is not perfect,” said Rochelle Walensky, chief of infectious diseases at Massachusetts General Hospital.
Robert Wachter, chairman of the University of California at San Francisco’s department of medicine, said any patient of his with Trump’s symptoms and treatment who wanted to be discharged from the hospital three days after their admission would need to sign out against doctors’ orders because it would be so ill-advised.
“For someone sick enough to have required remdesivir and dexamethasone, I can’t think of a situation in which a patient would be okay to leave on day three, even with the White House’s medical capacity,” Wachter said.
[editor’s note: this is a typical WaPo post without opposing viewpoints – frankly as biased as you can get. The President is not you or me – and can be surrounded by doctors so that he can execute his job in the proper surroundings]
Trump’s doctor defends his SUV ride yesterday – CNN
[editor’s note: because the mass media continues to slam Trump’s little ride outside the hospital yesterday – here is the rational from the medical side. Normally I would not cover crap like this but there is significant slanting in the media going on right now as we near voting day.]
President Trump’s physician Dr. Sean Conley was pressed by reporters on the question of why it was safe for him to leave Walter Reed medical center on Sunday for an SUV ride to wave to his supporters outside the facility.
Conley said that Trump “has been surrounded by medical and security staff for days wearing full PPE,” adding, “and yesterday the US Secret Service agents were in that same level of PPE for a very short period of time.
On the question of what precautions are being taken at the White House ahead of Trump’s planned return tonight, Conley said, “We worked with our infectious disease experts to make some recommendations for how to keep everything safe down at the White House for the President and those around him.”
He continued: “We’re looking at where he’s going to be able to carry out his duties, office space, and I’ll just say that it’s in line with everything we’ve been doing upstairs for the last several days.”
Inside the Flawed White House Testing Scheme That Did Not Protect Trump – Kaiser Health
President Donald Trump’s COVID-19 diagnosis is raising fresh questions about the White House’s strategy for testing and containing the virus for a president whose cavalier attitude about the coronavirus has persisted since it landed on American shores.
The president has said others are tested before getting close to him, appearing to hold it as an iron shield of safety. He has largely eschewed mask-wearing and social distancing in meetings, travel and public events, while holding rallies for thousands of often maskless supporters.
The Trump administration has increasingly pinned its coronavirus testing strategy for the nation on antigen tests, which do not need a traditional lab for processing and quickly return results to patients. But the results are less accurate than those of the slower PCR tests.
An early antigen test used by the White House was woefully inaccurate. But the new antigen test the White House is using has not been independently evaluated for accuracy and reliability. Moreover, this is the kit the Trump administration is pushing out to thousands of nursing homes to test residents and staff.
Testing “isn’t a ‘get out of jail free card,'” said Dr. Alan Wells, medical director of clinical labs at the University of Pittsburgh Medical Center and creator of its test for the novel coronavirus. In general, antigen tests can miss up to half the cases that are detected by polymerase chain reaction tests, depending on the population of patients tested, he said.
The FDA sent a warning letter to Nephron Pharmaceuticals for suggesting its budesonide inhalation solution could treat COVID-19 symptom – FDA
The FDA has issued a warning letter to Nephron Pharmaceuticals Corporation (Nephron) due to emails Nephron’s CEO and a sales representative sent concerning its product Budesonide Inhalation Suspension, which were the subject of complaints submitted to the FDA Bad Ad Program. The emails provide evidence that Budesonide is intended for a new use for which it lacks approval, specifically the treatment of symptoms associated with COVID-19, and for which its labeling does not provide adequate directions for use. This renders Budesonide misbranded within the meaning of the Federal Food, Drug, and Cosmetic Act (FD&C Act) and makes its distribution violative. The emails are also false or misleading in that they represent that Budesonide has certain benefits, but fail to include any risk information about the drug. This also renders Budesonide misbranded and makes its distribution violative. These violations are concerning because they create a misleading impression about the safety and effectiveness of Budesonide for the treatment of COVID-19 and suggest a use for which the labeling does not provide adequate directions for safe and effective use of the product.
A new culprit for severe COVID-19 cases – DDN
More than 10 percent of people who develop severe COVID-19 have misguided antibodies that attack not the virus, but the immune system itself, new research shows. Another 3.5 percent, at least, carry a specific kind of genetic mutation.
In both groups, the upshot is basically the same: The patients lack type I interferon, a set of 17 proteins crucial for protecting cells and the body from viruses. Whether the proteins have been neutralized by so-called auto-antibodies, or were not produced in sufficient amounts in the first place due to a faulty gene, their missing-in-action appears to be a common theme among a subgroup of COVID-19 sufferers whose disease has thus far been a mystery.
Published in two papers in Science, the findings help explain why some people develop a disease much more severe than others in their age group—including, for example, individuals who required admission to the ICU despite being in their 20s and free of underlying conditions. They may also provide the first molecular explanation for why more men than women die from the disease.
“These findings provide compelling evidence that the disruption of type I interferon is often the cause of life-threatening COVID-19,” said Jean-Laurent Casanova, head of the St. Giles Laboratory of Human Genetics of Infectious Diseases at The Rockefeller University and a Howard Hughes Medical Institute investigator. “And at least in theory, such interferon problems could be treated with existing medications and interventions.”
US Schools in Suburbs, Small Cities Reopening Without COVID Spike; Big Cities Up Next – Reuters
U.S. schools from kindergarten to high school have avoided a spike in COVID-19 cases, early data show, but medical experts say the real test is coming as students in large densely-populated cities such as New York and Miami return to classrooms.
The Centers for Disease Control and Prevention this week said more than 270,000 COVID-19 cases had been reported in children aged 5-17 since March. Cases in school-age children ticked slightly higher in mid-September as more schools reopened, but remains well below the peak set in mid-July.
Over 700 primary, middle and high schools that have at least partially reopened, reported that 0.07% of students and 0.14% of staff had a confirmed coronavirus infection in the first half of September, according to data collected by Brown University bit.ly/3kWpwnJ.
While the Brown sample is a fraction of the United States, and national statistics are scarce, a study by Switzerland’s Insights for Education of 191 countries found reopening schools here is not linked to an increase in COVID-19 rates.
“There is starting to be some reassuring data that when you put in place the right measures – and have control of community spread … you can open schools safely,” said Dr. Nathaniel Beers, co-author of the American Academy of Pediatrics’ school opening guidelines.
Lessons for working in construction during a pandemic – The Hill
… As CDC guidelines evolved, the AOC further adapted. We provided daily communications to quickly establish processes and procedures and push them across the organization. Contractors were required to screen workers to prevent cases on sites, remove sick workers, immediately report potential COVID cases to the AOC and complete contact traces.
We implemented weekly fogging, or misting disinfectant, in high-traffic work areas. We also adjusted work schedules so that different trades are not working in close proximity to each other, reducing the risk of exposure. As we learned on the job and received new guidance from medical experts, we have continually strengthened our safety procedures.
With these preventive measures in place, the AOC is experiencing a steadily and increasingly lower transmission rate. When we do have an employee test positive, we’ve taken steps to protect those who work with that person and prevent further spread while keeping our vital projects on schedule. Our tracking process incorporates CDC guidance, providing timelines for quarantine and safe return for anyone who tests positive and for anyone who has come in contact with that person.
The following are foreign headlines with hyperlinks to the posts
Only higher-risk groups will get a coronavirus vaccine in Britain, according to the country’s vaccine task force chair.
WHO: 1 in 10 people worldwide may have been infected by coronavirus
Nearly 16,000 cases in the U.K. weren’t counted because of a spreadsheet glitch.
The following are additional national and state headlines with hyperlinks to the posts
Regal Movie Chain Will Close All 536 U.S. Theaters On Thursday
NYC To Close Businesses In Parts Of Brooklyn And Queens As Virus Takes Hold Again
Cuomo won’t approve closing businesses in 9 N.Y.C. hot spots, but will close schools on Tuesday.
White House press secretary Kayleigh McEnany and two aides have tested positive for coronavirus
Melania Trump reports ‘feeling good’ after coronavirus diagnosis
Biden Says It’s ‘Fine’ to Move Forward With Second Presidential Debate
North Carolina Teacher Becomes 8th Killed by COVID Since School Year Began
White House Tells Staff With COVID Symptoms to Stay Home
Rare Side Effect of Drug Given to Trump Includes Grandiose Delusions
‘Trump Defeats COVID’ Coin Goes on Sale at Unofficial White House Gift Shop
Substance Use Tied to Increased COVID-19 Risk
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
September 2020 ISM and Markit Services Surveys Remain Modestly In Expansion
September 2020 Conference Board Employment Index Improves But Remains Deep In Contraction
Federal Budgetary Effects Of Pandemic-Related Legislation
The Official Sectors Response To The Coronavirus Pandemic And Moral Hazard – Part 3 Of 3
Infographic Of The Day: The Uneven Pandemic Recovery Of U.S. Small Businesses
The Fed Checks Into The Hotel California
Coronavirus: Are Cases In England Really Slowing?
Market Catches Trump’s COVID Infection
Trump’s COVID-19 Diagnosis: What Lies Ahead Could Include A Constitutional Crisis Over Succession
Warning to Readers
The amount of politically biased articles on the internet continues to increase. And studies and opinions of the experts continue to contradict other studies and expert opinions. Honestly, it is difficult to believe anything anymore. A study usually cannot establish cause and effect – but only correlation. Be very careful what you believe about this pandemic.

I assemble this coronavirus update daily – sifting through the posts on the internet. I try to avoid politically slanted posts (mostly from CNN, New York Times, and the Washington Post) and can usually find unslanted posts on that subject from other sources on the internet. I wait to publish posts on subjects that I cannot validate across several sources. But after all this extra work, I do not know if I have conveyed the REAL facts. It is my job to provide information so that you have the facts necessary – and then it is up to readers to draw conclusions.
Coronavirus INTERACTIVE Charts
include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus.htm’); ?>
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19. At this point, herd immunity does not look like an option although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a higher death rate.
- There are at least 8 strains of the coronavirus. New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
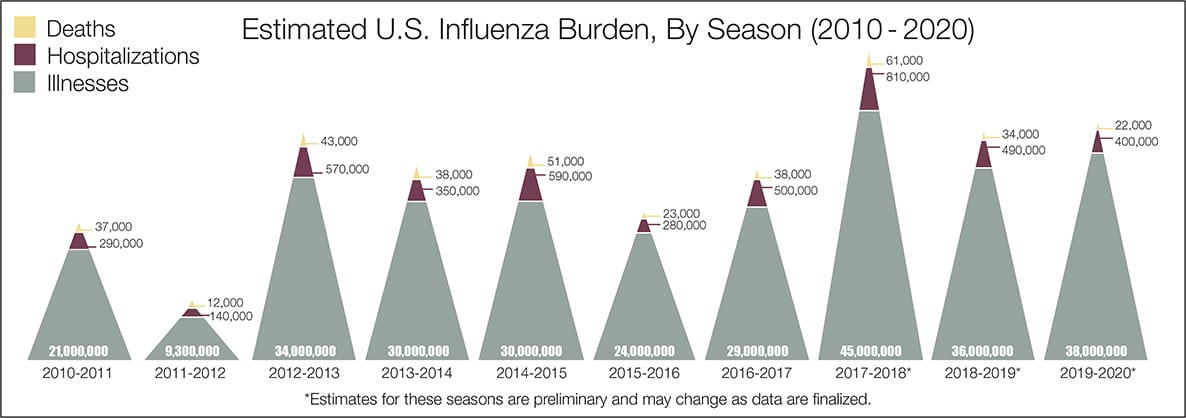
- The real question remains if the U.S. is over-reacting to this virus. The following graphic from the CDC puts the annual flu burden in perspective [click on image to enlarge]. Note that using this data is dangerous as the actual flu cases are estimated and not counted – nobody knows how accurate these guesses are.
What we do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work.
- Do we develop lasting immunity to the coronavirus? Another coronavirus – the simple cold – does not develop long term immunity.
- To what degree do people who never develop symptoms contribute to transmission?
- The US has scaled up coronavirus testing – and the accuracy of the tests has been improving. However, if one loses immunity – the coronavirus testing value is reduced.
- Can children widely spread coronavirus? [current thinking is that they are becoming a major source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- What effect will the weather have? At this point, it does not seem hot weather slows this coronavirus down – and it seems air conditioning contributes to its spread.
- Outdoor activities seem to be a lower risk than indoor activities.
- Can the world really push out an effective vaccine in 12 to 18 months?
- Will other medical treatments for Covid-19 ease symptoms and reduce deaths? So far only one drug (remdesivir) is approved for treatment.
- A current scientific understanding of the way the coronavirus works can be found [here].
Heavy breakouts of coronavirus have hit farm workers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of the respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>





