Written by Steven Hansen
The U.S. new cases 7-day rolling average is 1.6 % HIGHER than the 7-day rolling average one week ago. U.S. deaths due to coronavirus are now 4.6 % HIGHER than the rolling average one week ago. At the end of this post is a set of interactive graphs and tables for the world and individual States – as well as today’s headlines which include;
- Trump received an experimental antibody treatment from Regeneron.
- University of Texas in Trial Phase of Regeneron COVID Treatment Similar to Drug First Used by Trump
- The experimental coronavirus drug being used to treat President Trump has been trialed on hundreds of UK patients, and is “promising” and “potent”
- Remdesivir Treatment for Trump Costs More Than His Reported Tax Bill
- Trump team’s Covid-19 infections raise questions about coronavirus aboard Air Force One
- The next week is the critical phase in Trump’s illness. Here are the risks he faces.
- Want to reduce your COVID-19 risk? You need to sleep more.
- A ‘herd mentality’ can’t stop the COVID-19 pandemic. Neither can a weak vaccine.
- Multiple Demands Causing Women To Abandon Workforce
- Racial Minorities Hit Harder by Second Wave of COVID-19, Doctors Warn
​​ 
The recent worsening of the trendlines for new cases should be attributed to going back to school – especially at college/university level.
My continuing advice is to continue to wash your hands, wear masks, and maintain social distancing. No handwashing, mask, or social distancing will guarantee you do not get infected – but it sure as hell lowers the risk in all situations – and evidence to-date shows a lower severity of COVID-19. In addition, certain activities are believed to carry higher risk – like being inside in air conditioning and removing your mask (such as restaurants, around your children/grandchildren, bars, and gyms). It is all about viral load – and outdoor activities are generally very safe.
The daily number of new cases in the U.S. is remaining stubbornly and embarrassedly high.
The following graphs show the 7-day rolling average for new coronavirus cases and deaths have been updated through 03 October 2020:


z coronavirus.png​
Coronavirus Statistics For 03 October 2020 |
| U.S. Only | Global | U.S Percentage of Total | ||||
| Today*** | Cumulative | Today*** | Cumulative | Today | Cumulative | |
| New Confirmed Cases | 42,693 | 7,330,000 | 295,510 | 34,680,000 | 14.5% | 21.1% |
| Deaths** | 908 | 208,716 | 5,523 | 1,030,000 | 16.4% | 20.3% |
| Mortality Rate | 2.1% | 2.8% | 1.9% | 3.0% | ||
total COVID-19 Tests per 1,000 people | 0.92* | 345.84* | ||||
* as of 29 Sep 2020
** evidently several States included “probable” deaths today in the number
*** red color indicates record number
Coronavirus News You May Have Missed
Trump Gets Experimental COVID Tx – MedPage
Bloomberg reported that Trump would be staying at Walter Reed for “the next few days,” citing a statement from the White House.
An earlier statement from White House physician Sean Conley, DO, said the president had received “a single 8 gram dose of Regeneron’s polyclonal antibody cocktail,” which was completed “without incident.”
Regeneron had released topline results for its investigational REGN-COV2 antibody cocktail on Tuesday: the phase I/II/III trial showed the drug “reduced viral load and the time to alleviate symptoms in non-hospitalized patients with COVID-19,” as well as showing positive trends towards reducing medical visits.
But the product has not received FDA approval emergency use authorization yet, making it truly investigational. Some physicians on Twitter were puzzled that the president was using it. Jeremy Faust, MD, of Brigham and Women’s Hospital in Boston, tweeted that the president’s team either “can’t read basic medical literature” or “can read basic medical literature, but can’t overrule what [the president] is telling them to do” — or the president’s condition is far more serious than reported, and they are trying everything.
Trump is also receiving zinc, vitamin D, famotidine (Pepcid AC), melatonin, and a daily aspirin, according to Conley. It wasn’t clear whether these were started as COVID therapy or were simply part of his regular regimen. Conley also didn’t mention the president’s daily statin that had been reported on previously.
Conley said the president is “fatigued, but in good spirits,” and added that First Lady Melania Trump, who also tested positive, has “a mild cough and headache.”
[editor’s note: also read Trump received an experimental antibody treatment from Regeneron. Also, according to CNN: “The experimental coronavirus drug being used to treat President Trump has been trialed on hundreds of UK patients, and is “promising” and “potent,” according to an Oxford University professor.” ]
Trump’s Health Update Only Raises More Questions – MedPage
A brief press conference at Walter Reed Medical Center on Saturday sought to provide answers, but may only have raised more questions about President Trump’s clinical status since his COVID-19 diagnosis.
The main point of contention between White House physician Sean Conley, DO, and reporters was if the president ever received supplemental oxygen. Conley said the president’s last oxygen saturation level was 96 and the president “was not on any oxygen right now and has not needed any this morning, today at all.”
… When reporters pressed, Conley gave a hard no to supplemental oxygen on Thursday and Saturday, and said, “yesterday with the team while we were all there, he was not on oxygen.”
However, an AP source explicitly stated the president was administered supplemental oxygen on Friday before going to the hospital. CBS News reporter Sarah Cook also said via Twitter that a source familiar with the president’s health described the president’s vitals over the last 24 hours as “very concerning” and “the next 48 hours will be critical in terms of his care.”
Reporter Maggie Haberman of the New York Times added that two sources close to the president told her that his “blood oxygen levels dropped yesterday.”
… He noted the president has been fever-free for 24 hours, having had a fever on “Thursday and Friday morning,” though he would not specify how high the fever had been. Conley also said the president had been receiving daily ultrasounds and daily lab work.
One of Trump’s treating physicians, Brian Garibaldi, MD, of Johns Hopkins University, elaborated on the president’s course of treatment, saying the president received “special antibody therapy” 48 hours ago, and is currently on a 5-day course of remdesivir.
Sean Dooley, MD, of Walter Reed Medical Center, said the president’s cardiac function, kidney function and liver function are all normal.
A ‘herd mentality’ can’t stop the COVID-19 pandemic. Neither can a weak vaccine. – National Geographic
But even the trailblazers researching herd immunity were mystified by how to deploy it in practice. This conundrum has featured in battles against many modern plagues-such as smallpox, polio, and measles. And now it is part of the debate as the COVID-19 pandemic continues to flourish around much of the world.
Some prominent leaders wonder if herd immunity created as people are naturally infected with SARS-CoV-2 coronavirus would be enough to restore society to working order. For evidence, they point to hard-hit epicenters such as New York City, where approximately 20 percent of the residents have been infected and the caseload has been low and steady for months. This sustained recovery must be due to herd protection, they argue.
But based on simple math, past experiences with outbreaks, and emerging evidence from the ongoing pandemic, this claim is a fantasy.
… A vaccine with 50-percent efficacy could spare hundreds of thousands from hospitalizations, chronic health issues, and death-but it couldn’t hit the herd immunity threshold on its own even if everyone took it. The safest bet is a vaccine above 75 percent efficacy.
… Only two infectious diseases have ever been eradicated: the human scourge of smallpox and the cattle-borne germ rinderpest. All other known afflictions-including such Old World pestilences as rabies, leprosy, and bubonic plague-have either been managed through human intervention or remain uncontrolled.
[editor’s note: this is a great summary post on herd immunity and immunization – and deserves a full read]
The next week is the critical phase in Trump’s illness. Here are the risks he faces. – New York Times
… Older men are up to two times as likely to die from Covid-19, the disease caused by the coronavirus, as women of the same age, according to an analysis by the Chinese Center for Disease Control and Prevention. Another study, published in the journal Nature in August, found that the disparity was because men produce a weaker immune response than do women.
Dr. Nace said that 5 to 15 percent of men in their mid-70s die from coronavirus, although Mr. Trump, who is 74, will obviously benefit from excellent medical care. And he said doctors know a lot more about how to treat Covid-19 now than they did early in the pandemic.
“My big fear is that he probably had a greater exposure,” Dr. Nace said.

Want to reduce your COVID-19 risk? You need to sleep more. – National Geographic
“We have a lot of evidence that if you have an adequate amount of sleep, you definitely can help to prevent or fight any kind of infection,” says Monika Haack, a psychoneuroimmunologist at Harvard Medical School in Boston. “How many deaths can you prevent if you sleep properly, or how much less is the severity of your symptoms? I think that needs more research.”
Until a vaccine is available, the key to avoiding COVID-19 is reducing one’s risk of infection as much as possible. As new data roll in on sleep and this disease, scientists hope to better elucidate the complex workings of the immune system, while also providing clearer guidelines on how to use sleep as a weapon to stave off the pandemic.
Humans aren’t the only animals to benefit from sleep. Grisly studies from the late 1800s showed that when dogs and rats are completely deprived of sleep, the animals die within a couple weeks. For people, chronic sleep deprivation has long-term consequences, too, raising risks for type 2 diabetes, cardiovascular disease, dementia, and depression. Some of those chronic conditions are among the risk factors that increase susceptibility to COVID-19.
Enough Already: Multiple Demands Causing Women To Abandon Workforce – NPR
Here’s a stunning stat: Women are leaving the workforce at four times the rate as men.
The burden of parenting and running a household while also working a job during the pandemic has created a pressure cooker environment in many households, and women are bearing the brunt of it.
It has come to a head as a new school year starts with many children staying home instead of returning to their classrooms in person because of the pandemic. And its forcing many women to make a difficult choice and drop out of the workforce altogether.
Just in September, 865,000 women over 20 dropped out of the American workforce compared with 216,000 men in the same age group, the Labor Department reported Friday.
“It was a really startling difference,” said University of Michigan economist Betsey Stevenson. “The child care crisis is wreaking havoc on women’s employment.”
Point Mutation May Help Explain Different National COVID-19 Death Rates – Medscape
Ethnic differences in the frequencies of alpha-1 antitrypsin deficiency alleles might contribute to national differences in COVID-19 fatality rates, researchers report.
“It was interesting to see how one point mutation in a relevant gene can tell the difference on a national level between high and low mortality rates,” Dr. Noam Shomron of Tel Aviv University, in Israel, told Reuters Health by email.
Two single nucleotide polymorphisms (SNPs) in SERPINA1, which encodes alpha-1 antitrypsin, are responsible for antitrypsin deficiency in humans. The PiZ allele is associated with greater deficiency than the PiS allele. Earlier studies have identified higher COVID-19 infection rates among carriers than among non-carriers of PiZ.
Dr. Shomron and colleagues examined the possible association between the distributions of these SNPs and COVID-19 epidemiology across different regions of the world.
The PiZ allele was considerably less frequent in East and Southeast Asian populations (two alleles per 1,000 individuals) than in South European populations (17 alleles per 1,000 individuals). And the PiS allele showed even greater disparity, with five alleles versus 86 per 1,000, respectively, the researchers report in the FASEB Journal.
Covariance analysis revealed a significant positive association between estimated national alpha-1 antitrypsin deficiency (based on allele frequencies) and COVID-19 mortality rates after controlling for Human Development Index, urbanization level, volume of international travel, and proportions of elderly people.
Racial Minorities Hit Harder by Second Wave of COVID-19, Doctors Warn – Newsweek
Racial minorities are again being disproportionately impacted by COVID-19 in the U.K. and the government should urgently implement measures to mitigate against it, the British Medical Association (BMA) has warned.
The stark warning comes after U.K. Prime Minister Boris Johnson confirmed that a second wave of COVID-19 was taking place across the country, with the number of new cases being confirmed reaching above 7,000 this week.
Dr. Chaand Nagpaul, Chair of the Council of the BMA told Newsweek: “The same disproportionate impact on the Black, Asian and Minority Ethnic (BAME) community is still showing at the same level as at the beginning of April during the first peak.”
Public Health England (PHE) had previously commissioned a review to determine why people from BAME backgrounds were being disproportionally affected by the virus. The Office for National Statistics found in May that Black people are more than four times more likely to die from COVID-19 than white people.
Bangladeshi and Pakistani males were 1.8 times more likely to die from COVID-19 than white males, after pre-existing factors had been accounted for, with females from both ethnic groups 1.6 times more likely to die from the virus than their white counterparts.
A study commissioned by Mayor of London Sadiq Khan this week found that black people were 1.9 times more likely to die from COVID-19 than white people, with men of Pakinstani and Bangladeshi heritage are almost twice as likely to die.
White House rapid testing product is known to deliver incorrect results – New York Times
For months, the White House’s strategy for keeping President Trump and his inner circle safe has been to screen all White House visitors with a rapid test.
But the product they use, Abbott’s ID Now, was never intended for that purpose and is known to deliver incorrect results. In issuing an emergency use authorization, the Food and Drug Administration said the test was to be used only by a health care provider “within the first seven days of symptoms.”
The ID Now has several qualities in its favor: It’s portable, doesn’t need skilled technicians to operate and delivers results in 15 minutes. Used to evaluate someone with symptoms, the test can quickly and easily diagnose Covid-19, the disease caused by the coronavirus.
In people who are infected but not yet showing symptoms, however, the test is much less accurate, missing as many as one in three cases.
Trump team’s Covid-19 infections raise questions about coronavirus aboard Air Force One – CNN
Administration officials said Friday that presidential senior adviser Hope Hicks was showing coronavirus symptoms while she flew on the world’s most famous jet earlier this week, raising the concern her infection could be linked to the infections of President Donald Trump and first lady Melania Trump.
Experts have cautioned that during the pandemic, the unique air flow dynamics in the confined cabin of a jetliner — even one as large as the Boeing 747-200, known in the military as a VC-25 — could put unmasked passengers at a risk of catching the deadly virus.
Administration officials said Friday that Hicks began displaying symptoms on the flight back from the President’s Wednesday rally in Minnesota and was isolated in a separate cabin. She was seen deplaning Air Force One from a rear set of steps not typically used by the President.
“Social distancing is much easier on Air Force One than any commercial airliner,” said Professor Yan Chen of Purdue University, a researcher who studies the airborne spread of coronavirus inside an airliner. Chen said most passengers do not sit in cramped rows on board the multi-room, highly modified jet, “but complete isolation is very difficult.”
Chen said the air onboard large jets, including commercial airliners and Air Force One, is typically filtered through High Efficiency Particulate Air, or HEPA, filters, which are designed to catch most particles. The result is the air even on large planes is completely replaced every few minutes.
Air Force One also carries a special onboard oxygen system, although its capabilities aren’t clear.
Commercial airlines insist air filters make flying in a plane safer than sitting in a shared room in a building. But it does not eliminate the risk of contracting the virus when a contagious passenger is onboard.
University of Texas in Trial Phase of Regeneron COVID Treatment Similar to Drug First Used by Trump – Newsweek
Scientists are carrying out tests for a trial of a similar experimental antibody treatment than was first given to President Trump as he began treatment for the coronavirus.
UTHealth researchers are studying the efficacy of an antibody treatment from drug maker Eli Lilly as well as the first treatment of antibodies the president took, from Regeneron Pharmaceuticals.
Since being admitted to Walter Reed National Military Medical Center for further monitoring on Friday, specialists at the hospital opted to initiate Remdesivir therapy, according to a statement from the official presidential physician, Dr. Sean P. Conley.
“There’s been a history of using antibody’s to treat infections,” said Dr. Netanya Utay, Associate Professor of Internal Medicine at UTHealth. “The results that are out so far definitely look promising, but they’re from small trials.”
Here’s everything we know about the unapproved antibody drug Trump took to combat coronavirus – CNBC
Former Food and Drug Administration commissioner Dr. Scott Gottlieb told CNBC on Friday he believes the White House carefully considered all of its treatment options before it opted to give President Donald Trump the experimental coronavirus antibody cocktail from Regeneron Pharmaceuticals.
“This was a wholly appropriate decision to give him active therapy, and then it just became a choice of which therapy,” Gottlieb said on “Fast Money,” prior to Trump being taken to Walter Reed Medical Center “out of an abundance of caution” following his coronavirus diagnosis.
“I wouldn’t infer anything from the fact they chose the Regeneron product over another product – other than they probably had confidence looking at the data on the Regeneron product that it seemed to be the most effective of the products, given what they knew,” added Gottlieb, who led the regulatory agency under Trump from May 2017 to April 2019.
Not everyone in the medical community agrees with Gottlieb about the decision to give Trump an experimental treatment. Some shared concerns about the preferential treatment provided to the president, as the drug has not been approved by federal regulators, and others pointed to the limited available data.
On Tuesday, Regeneron said its REGN-COV2 treatment improved symptoms and reduced viral loads in non-hospitalized patients who have mild to moderate Covid-19. That was based on results for the first 275 trial patients. At the time, the company indicated it plans to “rapidly” discuss the early results with regulatory agencies, including the FDA.
Regeneron is not the only company developing antibody drugs; Eli Lilly and GlaxoSmithKline also are testing monoclonal antibodies, which experts have viewed as a promising potential Covid-19 treatment.
Regeneron’s REGN-COV2 is an experimental shot of lab-generated antibodies that mimics how the body would mount a reaction to a foreign invader. The goal is to boost the immune system’s defenses, rather than to wait on human biology to do its job.
Remdesivir Treatment for Trump Costs More Than His Reported Tax Bill – Newsweek
In June, the drugmaker behind the medication, Gilead Sciences, announced it would charge $520 per vial of remdesivir for patients with private insurance. This would make a five-day treatment course cost $3,120, although for developed countries outside the U.S. it would be nearly $800 cheaper. It would also cost less for Americans on certain government programs.
… Gilead has also faced criticism over the drug’s price, with Rep. Lloyd Doggett telling NPR in June that the taxpayer had taken the risk in its development. “Without a taxpayer investment of $99 million, this drug would have been abandoned.”
However, the Institute for Clinical and Economic Review, or ICER, which analyzes drug pricing, said Gilead had “made a responsible pricing decision based on the evidence we have today.” Newsweek has contacted Gilead for comment.
The following are foreign headlines with hyperlinks to the posts
Kim Jong Un says he wishes Trump a speedy recovery from COVID-19
The following are additional national and state headlines with hyperlinks to the posts
Trump campaign manager tests positive for COVID-19
Kellyanne Conway tests positive for COVID-19
Twitter to remove posts hoping for Trump’s death
GOP Sen. Thom Tillis tests positive for coronavirus
Controversial Doc is Furious Trump Took ‘Experimental Antibody Stupidness’
Regeron CEO Says Trump Will Recover in a Week Due to Experimental Drug
The president of Notre Dame tests positive, less than a week after a White House visit.
‘The likely outcome’: Trump’s COVID diagnosis followed waning precautions at the White House
New James Bond movie pushed to April 2021 as coronavirus cases continue to rise
After Republican COVID-19 positives, Senate to remain out until Oct. 19
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
Did The $600 Unemployment Supplement Discourage Work?
Expanding The Toolkit: Facilities Established To Respond To The COVID-19 Pandemic – Part 1 Of 3
This May Make You Rethink The Economic Recovery
The Fed’s Bazooka Is Broken – Will Direct Lending Be Next?
2021 To Set Off Avalanche Of Business Insolvencies
Warning to Readers
The amount of politically biased articles on the internet continues to increase. And studies and opinions of the experts continue to contradict other studies and expert opinions. Honestly, it is difficult to believe anything anymore. A study usually cannot establish cause and effect – but only correlation. Be very careful what you believe about this pandemic.

I assemble this coronavirus update daily – sifting through the posts on the internet. I try to avoid politically slanted posts (mostly from CNN, New York Times, and the Washington Post) and can usually find unslanted posts on that subject from other sources on the internet. I wait to publish posts on subjects that I cannot validate across several sources. But after all this extra work, I do not know if I have conveyed the REAL facts. It is my job to provide information so that you have the facts necessary – and then it is up to readers to draw conclusions.
Coronavirus INTERACTIVE Charts
include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus.htm’); ?>
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19. At this point, herd immunity does not look like an option although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a higher death rate.
- There are at least 8 strains of the coronavirus. New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
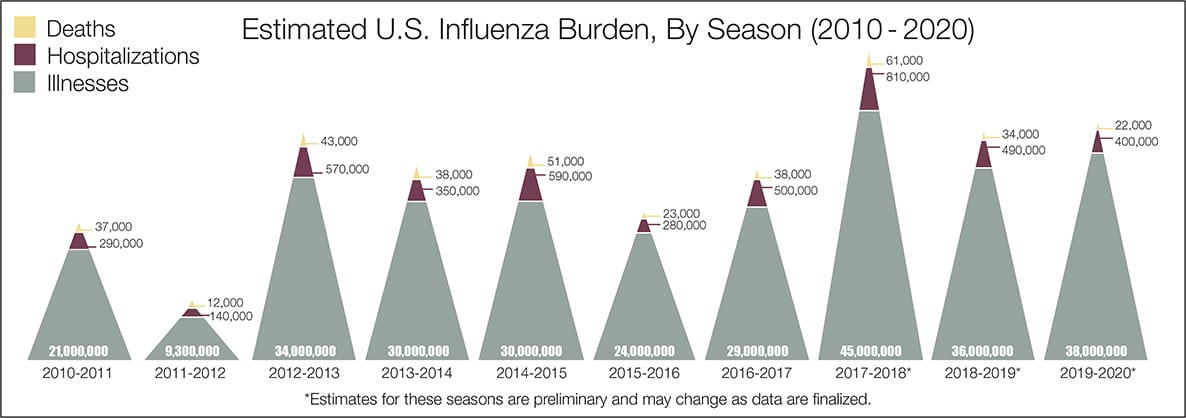
- The real question remains if the U.S. is over-reacting to this virus. The following graphic from the CDC puts the annual flu burden in perspective [click on image to enlarge]. Note that using this data is dangerous as the actual flu cases are estimated and not counted – nobody knows how accurate these guesses are.
What we do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work.
- Do we develop lasting immunity to the coronavirus? Another coronavirus – the simple cold – does not develop long term immunity.
- To what degree do people who never develop symptoms contribute to transmission?
- The US has scaled up coronavirus testing – and the accuracy of the tests has been improving. However, if one loses immunity – the coronavirus testing value is reduced.
- Can children widely spread coronavirus? [current thinking is that they are becoming a major source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- What effect will the weather have? At this point, it does not seem hot weather slows this coronavirus down – and it seems air conditioning contributes to its spread.
- Outdoor activities seem to be a lower risk than indoor activities.
- Can the world really push out an effective vaccine in 12 to 18 months?
- Will other medical treatments for Covid-19 ease symptoms and reduce deaths? So far only one drug (remdesivir) is approved for treatment.
- A current scientific understanding of the way the coronavirus works can be found [here].
Heavy breakouts of coronavirus have hit farm workers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of the respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>





