Written by Steven Hansen
The U.S. new cases 7-day rolling average is 12.0 % HIGHER than the 7-day rolling average one week ago. U.S. deaths due to coronavirus are now 5.8 % LOWER than the rolling average one week ago. At the end of this post is a set of interactive graphs and tables for the world and individual States – as well as today’s headlines which include;
- New coronavirus cases increased this past week in the U.S. and globally.
- Coronavirus deaths modestly declined this past week in the U.S. and modestly grew globally.
- The coronavirus infection this past week fatality rate worsened in the U.S. but remained constant globally.
- The Most Likely Way You’ll Get Infected With Covid-19
- COVID-19 Daily Cases On The Rise In Nearly Half Of U.S. States
- Regular UK lockdowns could help control Covid, says Sage expert

The recent worsening of the trendlines for new cases should be attributed to going back to school – especially at college/university level.
My continuing advice is to continue to wash your hands, wear masks, and maintain social distancing. No handwashing, mask, or social distancing will guarantee you do not get infected – but it sure as hell lowers the risk in all situations – and evidence to-date shows a lower severity of COVID-19. In addition, certain activities are believed to carry higher risk – like being inside in air conditioning and removing your mask (such as restaurants, around your children/grandchildren, bars, and gyms). It is all about viral load – and outdoor activities are generally very safe.
The daily number of new cases in the U.S. is remaining stubbornly and embarrassedly high.
The following graphs show the 7-day rolling average for new coronavirus cases and deaths have been updated through 27 September 2020:


z coronavirus.png
Coronavirus Statistics For 27 September 2020 |
| U.S. Only | Global | U.S Percentage of Total | ||||
| Today*** | Cumulative | Today*** | Cumulative | Today | Cumulative | |
| New Confirmed Cases | 44,833 | 7,080,000 | 296,556 | 32,920,000 | 15.1% | 21.5% |
| Deaths** | 723 | 204,497 | 5,414 | 995,147 | 13.4% | 20.5% |
| Mortality Rate | 1.6% | 2.9% | 1.8% | 3.0% | ||
total COVID-19 Tests per 1,000 people | 0.91* | 324.17* | ||||
* as of 22 Sep 2020
** evidently several States included “probable” deaths today in the number
*** red color indicates record number
A Summary of this Past Week
New coronavirus cases increased this past week in the U.S. and globally.

Coronavirus deaths modestly declined this past week in the U.S. and modestly grew globally.

The coronavirus infection this past week fatality rate worsened in the U.S. but remained constant globally.

Econintersect published today two posts that summarize the coronavirus headlines this week:
How Will We Judge The Real Effectiveness Of Any Vaccine?
According to Massachusetts General Hospital, there are two questions that scientists must answer in order to successfully develop a vaccine:
- Is there evidence of natural protective immunity to SARS-CoV-2 after an individual has been infected and recovered?
- Is there evidence that a vaccine can induce immunity in subjects who have not been exposed to the virus, and if so, what does that look like in terms of types and numbers of antibodies?
The current vaccine trials underway divide their guinea pigs into two groups – one group given the real vaccine and another group given a placebo. It is the comparison between the groups which would determine the effectiveness of the vaccine.
The groups are too small to accurately judge hospitalization and death rates – which are the most important criteria. Getting sick and recovering is not all that important – getting sick, being hospitalized, or dying is very important.
According to the CDC, “The overall cumulative COVID-19 hospitalization rate is 174.8 per 100,000, with the highest rates in people aged 65 years and older (472.3 per 100,000) and 50-64 years (261.5 per 100,000).” This means that less than 0.2% of the population have been hospitalized due to coronavirus.
But looking at cumulative rates misses the target – the vaccine trials are over a short period – and the virus has evolved to a less deadly but more contagious version. In the last month, the hospitalization rate was 0.012% of the total U.S. population. With a sample size of 50,000, one would expect 6 people to be hospitalized each month. This would only be 3 people in each trial group (real vs placebo). With a sample size this small, it would be nearly impossible to judge the hospitalization effectiveness of any vaccine.
And the death number is much smaller as the small sample size would make a determination of the effectiveness of any vaccine impossible.
This leaves the important issues of the real effectiveness of the vaccine for hospitalization and death to all the people who initially take the approved vaccine(s).
The first groups that take the vaccine (health care workers, old people, and vulnerable Americans) the real guinea pigs – this is not logical.
In my opinion, with the size of the guinea pig groups so small – the ONLY way to judge the effectiveness of any vaccine is to expose all the guinea pigs to COVID-19.
Coronavirus News You May Have Missed
The Most Likely Way You’ll Get Infected With Covid-19 – Medium
Surfaces don’t seem to matter as much as originally thought …It turns out that despite the catastrophic harm it’s caused, the novel coronavirus is actually quite fragile, and it doesn’t like being out in the open where it can dry up. According to the NEJM paper, the virus’s half-life is a relatively short six hours, meaning that every six hours 50% of the virus shrivels up and becomes inactive or noninfectious. That means if you start with 100 virus particles, after six hours that number halves to 50 particles; six hours later there are 25 virus particles left, and fewer than 10 virus particles remain after 24 hours. However, if there are huge quantities of virus to start, many more will be left behind after each six-hour window, and it will take longer for all of the virus to disintegrate.
Close range droplets are the new leading theory … When you expel air — whether it’s by sneezing, coughing, talking, singing, shouting, or even breathing — tiny bits of saliva, ranging in size from an imperceptible mist to visible spittle, are pushed out. Heavier particles fall to the ground relatively quickly and are categorized as droplets, while the tinier particles stay afloat in the air for longer. When talking and breathing, the typical droplet trajectory is about three to six feet, hence the six-foot distancing recommendation. If the droplets are expelled with more force, like with a sneeze or a cough, they can travel further before hitting the earth.
Aerosol transmission has gradually gained acceptance … So if the novel coronavirus is airborne, why isn’t it as contagious as measles? One reason could be that measles is a hardier virus (remember that SARS-CoV-2 is relatively fragile) and can survive longer in those tiny aerosols. Another potential difference is the infectious dose — the amount of virus required to start an infection. Scientists still don’t know exactly how much of the novel coronavirus is needed to make someone sick, but it’s likely higher than conventional airborne viruses.
COVID-19 Daily Cases On The Rise In Nearly Half Of U.S. States – NPR
The number of new daily coronavirus infections in the U.S. continued to rise this past week, driven by upward trends in nearly half the states that have pushed total cases in the country past 7 million. At the same time, a recent study suggests the vast majority of Americans haven’t been exposed, far below what’s required to quell the virus’s spread through “herd immunity.”
Daily cases were largely on a downward trend through August and early September from highs in July, but are now going up again.
According to the Johns Hopkins University Coronavirus Tracker, the U.S. reported more than 55,000 new cases on Friday. In total, the U.S. has more than 7,074,000 infections with 204,000 dead as a result of COVID-19.
Overall, about two-dozen states and territories reported an upward trend in new infections, with some states setting and breaking records in days.
Regular UK lockdowns could help control Covid, says Sage expert – The Guardian
“A circuit breaker, or mini-lockdown can be used to reset the clock,” he told the Observer. “The idea would be to bring the incidence back to what it was a few weeks earlier. You replace two weeks of exponential growth with two weeks of a decline in cases. This can have a big effect on the total number of cases, particularly if it is implemented shortly after the epidemic starts to grow.
“To maximise the effect you also need longer-term measures to slow growth – perhaps along the lines of what Scotland has done. It is of course possible to do more than one circuit breaker – perhaps one now and one around half term. This could help reduce cases and deaths and – as the measures are short-lived and can be planned for – potentially limit the impact on the economy.”
The following are foreign headlines with hyperlinks to the posts
Israel heads into Yom Kippur with a worrying surge of cases.
The French Open, forced to move to autumn, debuts some useful added features.
Antarctica, the only continent without coronavirus, braces for summer rotation
The following are additional national and state headlines with hyperlinks to the posts
New York Reports Over 1,000 New COVID Cases for First Time in 113 Days
Office real estate market will get back to pre-Covid level, in 2025: Cushman & Wakefield
Cal State Long Beach halts in-person classes and locks down campus after positive Covid-19 tests
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
How Did State Reopenings Affect Small Businesses?
America’s Scariest Charts – Updated 27 September 2020
Shocking Chart On Low Income Consumers
Coronavirus Disease Weekly News 27September 2020
Coronavirus Economic Weekly News 27September 2020
Great Reset Update: $50 Trillion Debt Coming
How COVID-19 Is Changing The English Language
Warning to Readers
The amount of politically biased articles on the internet continues to increase. And studies and opinions of the experts continue to contradict other studies and expert opinions. Honestly, it is difficult to believe anything anymore. A study usually cannot establish cause and effect – but only correlation. Be very careful what you believe about this pandemic.

I assemble this coronavirus update daily – sifting through the posts on the internet. I try to avoid politically slanted posts (mostly from CNN, New York Times, and the Washington Post) and can usually find unslanted posts on that subject from other sources on the internet. I wait to publish posts on subjects that I cannot validate across several sources. But after all this extra work, I do not know if I have conveyed the REAL facts. It is my job to provide information so that you have the facts necessary – and then it is up to readers to draw conclusions.
Coronavirus INTERACTIVE Charts
include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus.htm’); ?>
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19. At this point, herd immunity does not look like an option although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a higher death rate.
- There are at least 8 strains of the coronavirus. New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
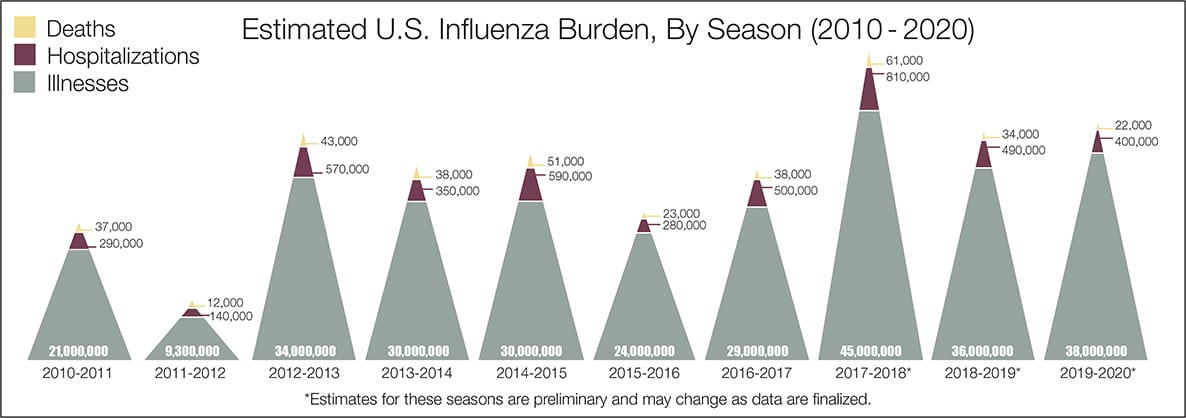
- The real question remains if the U.S. is over-reacting to this virus. The following graphic from the CDC puts the annual flu burden in perspective [click on image to enlarge]. Note that using this data is dangerous as the actual flu cases are estimated and not counted – nobody knows how accurate these guesses are.
What we do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work.
- Do we develop lasting immunity to the coronavirus? Another coronavirus – the simple cold – does not develop long term immunity.
- To what degree do people who never develop symptoms contribute to transmission?
- The US has scaled up coronavirus testing – and the accuracy of the tests has been improving. However, if one loses immunity – the coronavirus testing value is reduced.
- Can children widely spread coronavirus? [current thinking is that they are becoming a major source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- What effect will the weather have? At this point, it does not seem hot weather slows this coronavirus down – and it seems air conditioning contributes to its spread.
- Outdoor activities seem to be a lower risk than indoor activities.
- Can the world really push out an effective vaccine in 12 to 18 months?
- Will other medical treatments for Covid-19 ease symptoms and reduce deaths? So far only one drug (remdesivir) is approved for treatment.
- A current scientific understanding of the way the coronavirus works can be found [here].
Heavy breakouts of coronavirus have hit farm workers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of the respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>





