Written by Steven Hansen
The U.S. new cases 7-day rolling average is 12.3 % lower than the 7-day rolling average one week ago. U.S. deaths due to coronavirus are now 10.3 % lower than the rolling average one week ago. At the end of this post is a set of interactive graphs and tables for the world and individual States – as well as today’s headlines which include;
- New cases declined this week in the U.S. but marginally grew in the World.
- Coronavirus deaths declined in the U.S. but grew in the World.
- The coronavirus infection fatality rate improved in the U.S. but declined globally.
- Can Europe tame the pandemic’s next wave?
- COVID-19: Saving thousands of lives and trillions in livelihoods
- AstraZeneca Resumes Its COVID-19 Vaccine Trials In The U.K.
- It’s Not Easy to Get a Coronavirus Test for a Child
- Long-Term Care Policy after Covid-19 – Solving the Nursing Home Crisis
- Socioeconomic vulnerability increases the risk of dying from COVID-19

My continuing advice is to continue to wash your hands, wear masks, and maintain social distancing. No handwashing, mask, or social distancing will guarantee you do not get infected – but it sure as hell lowers the risk in all situations – and evidence to-date shows a lower severity of COVID-19. In addition, certain activities are believed to carry higher risk – like being inside in air conditioning and removing your mask (such as restaurants, around your children/grandchildren, bars, and gyms). It is all about viral load – and outdoor activities are generally very safe.
The daily number of new cases in the U.S. is remaining stubbornly and embarrassedly high.
The following graphs show the 7-day rolling average for new coronavirus cases and deaths have been updated through 13 September 2020:


z coronavirus.png
Coronavirus Statistics For 13 September 2020 |
| U.S. Only | Global | U.S Percentage of Total | ||||
| Today*** | Cumulative | Today*** | Cumulative | Today | Cumulative | |
| New Confirmed Cases | 34,320 | 6,490,000 | 268,757 | 28,800,000 | 12.8% | 22.5% |
| Deaths** | 685 | 193,701 | 4,926 | 920,931 | 13.9% | 21.0% |
| Mortality Rate | 2.0% | 3.0% | 1.8% | 3.2% | ||
total COVID-19 Tests per 1,000 people | 1.39* | 286.20* | ||||
* as of 08 Sep 2020
** evidently several States included “probable” deaths today in the number
*** red color indicates record number
A Review Of Last Week
New cases declined in the U.S. but marginally grew in the World.

Coronavirus deaths declined in the U.S. but grew in the World.

And the coronavirus infection fatality rate improved in the U.S. but declined globally.

And for a review of last week’s news, Econintersect published two posts today:
Where Are We Headed In This Pandemic Without Knowing The Real Facts?
Houston – We have a problem. The coronavirus won’t go away, and without it going away — the economy cannot completely recover and people are still dying from COVID-19. Many are pinning their pandemic forecasts on a vaccine or magic pill to make this pandemic go away.
To forecast the effect on people’s lives and the economy, we need to really understand the virus ignoring all the bullshit. Almost every day I publish expert’s opinion or study contradicted by another expert’s opinion or study.
The Republicans want to minimize pandemic whilst the Democrats want to exaggerate the pandemic. I find almost no one in politics is telling you the “truth” – nor are they taking steps to understand whatever the “truth” is.
And then we have the social media which believes they know the facts and block alternate views. Only a fool believes they know the facts about this pandemic.
Anyone can make good decisions IF they understand all the facts. Normally in business, decisions are made with 80 % to 90 % of the real facts. In this pandemic – there are few real facts known and most things the experts are telling us are extrapolations, unvetted theory, and anecdotal information. Honestly, I trust experts less than politicians as at least I understand politicians’ biases.

I assemble this coronavirus update daily – sifting through the posts on the internet. I try to avoid politically slanted posts (mostly from CNN, New York Times, and the Washington Post) and can usually find unslanted posts on that subject from other sources on the internet. I wait to publish posts on subjects that I cannot validate across several sources. But after all this extra work, I do not know if I have conveyed the REAL facts. It is my job to educate so that you have the facts necessary – and then it is up to readers to draw conclusions.
Like going to war, the pandemic response to date is chaotic. Decisions are being made in the absence of real facts. The experts are far from agreement.
One of the greatest mobilizations in U.S. history was World War II. It takes time to mobilize and begin to understand your opponent. It is trial and error – and most servicemen who fought in WWII talked about the chaos.

Source: http://ohhitsww2.weebly.com/timeline-of-the-important-events-of-world-war-two.html
We are smarter than we were 6 months ago – but not smart enough to make the pandemic go away. It took 4 years for the U.S. to stop WWII with literally 100% concentration on the war effort. I hope the pandemic can be stopped quickly, but I doubt life as we knew it can return within the next 12 months. Here, I hope it is me who does not understand what it takes to find a solution to the pandemic – and then execute an effective solution for the 7.6 billion people on planet Earth.
Life and the economy cannot return to “normal” until the pandemic is defeated.
Coronavirus News You May Have Missed
Can Europe tame the pandemic’s next wave? – Science
Drosten, of the Charité University Hospital in Berlin, is one of many calling for renewed vigilance, and he and others are urging a new control strategy that trades blanket lockdowns for measures specifically targeting clusters of cases, which play a key role in spreading the coronavirus. “We successfully aborted the [first] wave and now we should make sure that no new wave builds,” says epidemiologist Christian Althaus of the University of Bern.
Few dispute that Europe rose to the initial challenge. In Bergamo, a hotspot in Italy’s Lombardy region, crematoria were so overburdened in March that army trucks had to transport the dead to other cities—but on 24 May, Lombardy registered zero COVID-19 deaths for the first time. By early July, the European Union and the United Kingdom together averaged fewer than 5000 new cases per day, whereas the United States and Brazil (which together have roughly the same population) had 50,000 and 40,000, respectively. Europeans enjoyed a surprisingly normal summer, with northern Europeans flocking to Mediterranean beaches.
The rising case numbers today aren’t quite comparable to the peak in April because countries are now testing far more people on a daily basis. But the increase shows that Europe relaxed measures too early and too much, says virologist Ab Osterhaus of the University of Veterinary Medicine in Hanover, Germany. “The wrong message was given, basically: We have done a great job and now we can relax again.” Instead, Europe could have tried to emulate New Zealand by stopping community transmission completely and zealously guarding against reintroductions, says Devi Sridhar, a global health expert at the University of Edinburgh who has been advising the Scottish government. Scotland committed early on to pushing case numbers down to zero, but other countries did not, and now almost all are seeing a resurgence.
… Meanwhile, new insights into viral spread are leading to better targeted control measures. The emphasis on hand hygiene is gone because it has become clear that contaminated surfaces don’t play a large role. In the spring, some countries banned almost any outdoor activity, including jogging; now, the focus is on indoor activities. “We’ve learned outdoor hospitality is generally fine, nonessential shops are fine as long as people wear face coverings, public transport doesn’t seem that risky,” Sridhar says.
Instead, public health experts increasingly argue for targeting clusters of cases and superspreading events. Some studies estimate that 10% of patients cause 80% of all infections, whereas most don’t infect anybody at all. Drosten has urged that contact tracers spend more time finding the source of a new case—along with that person’s contacts—than the new case’s contacts; after all, the patient may not infect anybody else, but is likely to have caught the virus as part of a cluster, Drosten says.
[editor’s note: hard to summarize this post – it deserves a full read]
COVID-19: Saving thousands of lives and trillions in livelihoods – McKinsey
On March 23, 2020, McKinsey introduced the twin imperatives of safeguarding our lives and our livelihoods and a nine-scenario framework to describe potential economic and COVID-19 outcomes (Exhibit 1). At the time, we wrote that the best combined outcomes depended on a rapid and effective public-health response that controlled the spread of the novel coronavirus within two to three months. Similarly, in May, we wrote that crushing uncertainty by reducing the virus spread to near zero was likely the big “unlock” for most economies.
… Our new research looking for visible indicators of economic activity that would suggest such a rebound in growth finds them only in the countries that have successfully placed the virus under control. The evidence heavily suggests that a multifaceted public-health response that goes well beyond a simple transient lockdown is a necessary first step to restore confidence and create the conditions for growth.
It won’t be cheap: the cost of getting the virus under control is likely measured in the billions, or perhaps hundreds of billions, of dollars. But it is also clear that the opportunity cost of waiting is almost surely measured in unknown thousands of lives and trillions of dollars. The impact of delay is not linear. For every three months we delay in getting the virus under control, we push back the return of GDP to precrisis levels by about six months. Time is the enemy of both lives and livelihoods.
[editor’s note: another good think piece which deserves a full read]

AstraZeneca Resumes Its COVID-19 Vaccine Trials In The U.K. – NPR
Drugmaker AstraZeneca announced Saturday that its COVID-19 vaccine studies have resumed in the United Kingdom, though not yet in the United States. The vaccine trials had been placed on hold around the world earlier in the week after a U.K. participant in one of the studies developed a neurological illness.
The candidate vaccine was developed by the University of Oxford along with AstraZeneca. The goal of the large studies is to see whether the vaccine is capable of preventing COVID-19 and whether it is safe.
Although initial studies didn’t reveal serious side effects from the vaccine, rare complications of any vaccine, if there are any, may not turn up until it has been administered to thousands, or tens of thousands of people.
… According to a statement Saturday from the drug company, the studies were paused “to allow review of safety data by independent committees, and international regulators.”
The statement goes on to say that the committee has concluded its investigations and advised the Medicines Healthcare Products Regulatory Authority, the U.K. equivalent of the Food and Drug Administration, that trials in the U.K. are safe to resume.
It’s Not Easy to Get a Coronavirus Test for a Child – New York Times
As child care centers and schools reopen, parents are encountering another coronavirus testing bottleneck: Few sites will test children. Even in large cities with dozens of test sites, parents are driving long distances and calling multiple centers to track down one accepting children.
The age policies at testing sites reflect a range of concerns, including differences in health insurance, medical privacy rules, holes in test approval, and fears of squirmy or shrieking children.
The limited testing hampers schools’ ability to quickly isolate and trace coronavirus cases among students. It could also create a new burden on working parents, with some schools and child care centers requiring symptomatic children to test negative for coronavirus before rejoining class.
“There is no good reason not to do it in kids,” said Sean O’Leary, a Colorado pediatrician who sits on the American Academy of Pediatrics’ committee on infectious diseases. “It’s a matter of people not being comfortable with doing it.”
Many testing sites, including those run by cities and states, do not test any children, or they set age minimums that exclude young children. The age limits vary widely from place to place. Los Angeles offers public testing without any age minimum, while San Francisco, which initially saw only adults, recently began offering tests to children 13 and older. Dallas sets a cutoff at 5 years old.
Long-Term Care Policy after Covid-19 — Solving the Nursing Home Crisis – New England Journal of Medicine
Since the U.S. coronavirus outbreak began in a nursing home in Kirkland, Washington, more than 153,000 residents and employees of 7700 U.S. nursing homes have contracted Covid-19, accounting for 35% of the country’s deaths. Here, as in many other countries, nursing homes have been ill equipped to stop the spread of the virus. They lacked the resources necessary to contain the outbreak, including tests and personal protective equipment, and their staff are routinely underpaid and undertrained. Furthermore, nursing homes were sitting ducks for Covid-19, housing people who are particularly vulnerable to poor outcomes of the virus, often in shared living quarters and communal spaces, making social distancing or isolation difficult, if not impossible.
But this crisis in nursing homes is not a new problem. Long-term care in the United States has been marginalized for decades, leaving aging adults who can no longer care for themselves at home reliant on poorly funded and insufficiently monitored institutions. Although major regulatory policies, including the Federal Nursing Home Reform Act of 1987, have attempted to address deficiencies in the quality of care, Covid-19 has highlighted the fact that better monitoring is not enough. The coronavirus has exposed and amplified a long-standing and larger problem: our failure to value and invest in a safe and effective long-term care system.
Indeed, long-term care has been sidelined in our federal social welfare policies since the 1960s, when Medicare and Medicaid created narrow and incomplete social insurance programs for such care. These programs adopted a medicalized model of care, prioritizing the use of licensed providers and institutions. This model made nursing homes the default provider of long-term care and made the care provided by families and others outside these licensed facilities invisible, leaving it unsupported.
Furthermore, Medicare and Medicaid were never intended to pay for the lion’s share of long-term care. Medicare funds long-term care only temporarily and tangentially by covering nursing home-based rehabilitation after a hospital discharge. Medicaid finances more than half of all long-term care for people who need help with daily activities, such as bathing, dressing, or eating, but it’s available only to people who have spent down their own assets, and it has coverage gaps.
[editor’s note: this post deserves a full read]
Socioeconomic vulnerability increases the risk of dying from COVID-19 – McKinsey
People who have severe housing problems—or who are unemployed, incarcerated, or impoverished—are more vulnerable to contracting the novel coronavirus than the general population. They’re also more likely to have underlying health conditions that could make a case of COVID-19 more severe.
To read the report, see “US Hispanic and Latino lives and livelihoods in the recovery from COVID-19,” September 2, 2020.

The following are foreign headlines with hyperlinks to the posts
No new Canadian COVID-19 deaths reported for first time since mid-March
Global food security: When America leads, lives are saved
South Korea eases restrictions, and protesters in Australia call for the same.
The following are additional national and state headlines with hyperlinks to the posts
I tested positive for Covid-19 antibodies — what now?
Coronavirus Tests Are Supposed to Be Free. The Surprise Bills Come Anyway.
Temperature checks, required in many public places, have little value, U.S. health officials say.
Michigan State University students asked to self-quarantine after Covid-19 outbreak
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
Supporting Migrants And Remittances As COVID-19 Rages On
Is The COVID-19 Pandemic A Supply Or A Demand Shock?
U.S. Labor Market Shows Signs Of Recovery
On The Question Of Current And Future Lockdowns
Coronavirus Disease Weekly News 13September 2020
Coronavirus Economic Weekly News 13September 2020
Coronavirus INTERACTIVE Charts
include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus.htm’); ?>
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19. At this point, herd immunity does not look like an option although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a higher death rate.
- There are at least 8 strains of the coronavirus. New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
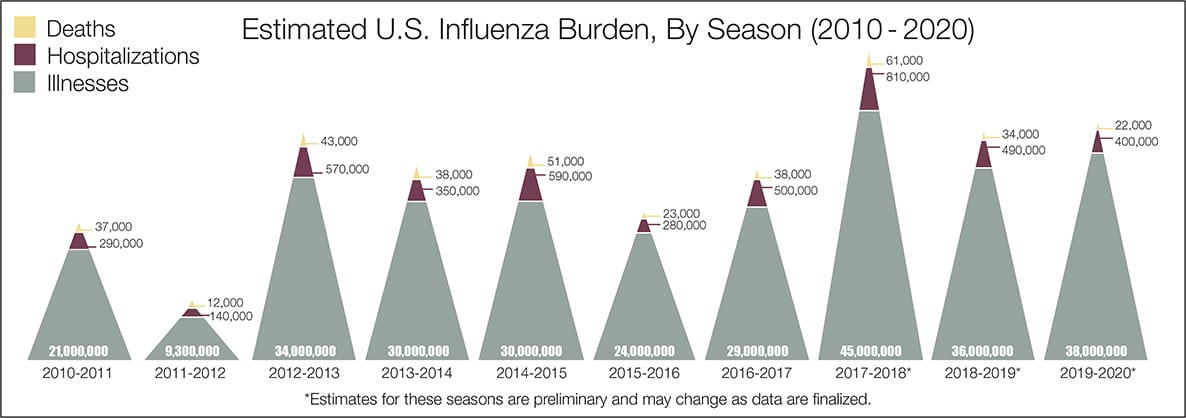
- The real question remains if the U.S. is over-reacting to this virus. The following graphic from the CDC puts the annual flu burden in perspective [click on image to enlarge]. Note that using this data is dangerous as the actual flu cases are estimated and not counted – nobody knows how accurate these guesses are.
What we do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work.
- Do we develop lasting immunity to the coronavirus? Another coronavirus – the simple cold – does not develop long term immunity.
- To what degree do people who never develop symptoms contribute to transmission?
- The US has scaled up coronavirus testing – and the accuracy of the tests has been improving. However, if one loses immunity – the coronavirus testing value is reduced.
- Can children widely spread coronavirus? [current thinking is that they are becoming a major source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- What effect will the weather have? At this point, it does not seem hot weather slows this coronavirus down – and it seems air conditioning contributes to its spread.
- Outdoor activities seem to be a lower risk than indoor activities.
- Can the world really push out an effective vaccine in 12 to 18 months?
- Will other medical treatments for Covid-19 ease symptoms and reduce deaths? So far only one drug (remdesivir) is approved for treatment.
- A current scientific understanding of the way the coronavirus works can be found [here].
Heavy breakouts of coronavirus have hit farm workers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of the respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>





