Written by Steven Hansen
The U.S. new cases 7-day rolling average is 2.5 % lower than the 7-day rolling average one week ago. U.S. deaths due to coronavirus are now 11.9 % lower the rolling average one week ago. At the end of this post is a set of interactive graphs and tables for the world and individual states – as well as today’s headlines which include;
- Don’t just look at covid-19 fatality rates. Look at people who survive – but don’t entirely recover.
- Thousands of students, staff sent home nationwide as COVID snarls school reopenings
- Hybrid schooling could be a public health disaster, some doctors warn
- Trump has found a new doctor for his coronavirus task force
- Health providers’ scramble for staff and supplies reveals sharp disparities
- CDC asks 4 states and a city to draft coronavirus vaccine distribution plans
- New research shows that gaiters can protect just as well as other cloth masks
- Dr. Scott Gottlieb: Yale’s new saliva coronavirus test funded by NBA could be widely rolled out

My continuing advice is to continue to wash your hands, wear masks, and maintain social distancing. No handwashing, mask, or social distancing will guarantee you do not get infected – but it sure as hell lowers the risk in all situations. In addition, certain activities are believed to carry higher risk – like being inside in air conditioning and removing your mask (such as restaurants, around your children/grandchildren, bars, and gyms). It is all about viral load.
The daily number of new cases in the U.S. is remaining stubbornly and embarrassedly high.
The following graphs show the 7-day rolling average for new coronavirus cases and deaths have been updated through 17 August 2020:


z coronavirus.png
Coronavirus Statistics For 17 August 2020 |
| U.S. Only | Global | U.S Percentage of Total | ||||
| Today*** | Cumulative | Today*** | Cumulative | Today | Cumulative | |
| New Confirmed Cases | 51,200 | 5,400,000 | 215,731 | 21,690,000 | 23.7% | 24.9% |
| Deaths** | 571 | 170,052 | 4,186 | 770,273 | 13.6% | 22.1% |
| Mortality Rate | 1.1% | 3.1% | 1.9% | 3.6% | ||
total COVID-19 Tests per 1,000 people | 2.35* | 202.32* | ||||
* as of 16 Aug 2020
** evidently several states included “probable” deaths today in the number
*** red color indicates record number
Coronavirus News You May Have Missed
Don’t just look at covid-19 fatality rates. Look at people who survive – but don’t entirely recover. – Washington Post
But with more data, something else has become clear: We’re focusing too much on fatality rates and not enough on the people who don’t die, but don’t entirely recover, either.
Anecdotal reports of these people abound. At least seven elite college athletes have developed myocarditis, an inflammation of the heart muscle that can have severe consequences, including sudden death. An Austrian doctor who treats scuba divers reported that six patients, who had only mild covid-19 infections, seem to have significant and permanent lung damage. Social media communities sprang up of people who are still suffering, months after they were infected, with everything from chronic fatigue and “brain fog” to chest pain and recurrent fevers.
Now, data is coming in behind the anecdotes, and while it’s preliminary, it’s also “concerning,” says Clyde Yancy, chief of cardiology at Northwestern University’s Feinberg School of Medicine. A recent study from Germany followed up with 100 recovered patients, two-thirds of whom were never sick enough to be hospitalized. Seventy-eight showed signs of cardiac involvement, and MRIs indicated that 60 of them had ongoing cardiac inflammation, even though it had been at least two months since their diagnosis.
If these results turned out to be representative, they would utterly change the way we think about covid-19: not as a disease that kills a tiny percentage of patients, mostly the elderly or the obese, the hypertensive or diabetic, but one that attacks the heart in most of the people who get it, even if they don’t feel very sick. And maybe their lungs, kidneys or brains, too.
The Plan That Could Give Us Our Lives Back – The Atlantic
Michael Mina is a professor of epidemiology at Harvard, where he studies the diagnostic testing of infectious diseases. He has watched, with disgust and disbelief, as the United States has struggled for months to obtain enough tests to fight the coronavirus. In January, he assured a newspaper reporter that he had “absolute faith” in the ability of the Centers for Disease Control and Prevention to contain the virus. By early March, that conviction was in crisis. “The incompetence has really exceeded what anyone would expect,” he told The New York Times. His astonishment has only intensified since.
… Why has testing failed so completely? By the end of March, Mina had identified a culprit: “There’s little ability for a central command unit to pool all the resources from around the country,” he said at a Harvard event. “We have no way to centralize things in this country short of declaring martial law.” It took several more months for him to find a solution to this problem, which is to circumvent it altogether. In the past several weeks, he has become an evangelist for a total revolution in how the U.S. controls the pandemic. Instead of restructuring daily life around the American way of testing, he argues, the country should build testing into the American way of life.
The wand that will accomplish this feat is a thin paper strip, no longer than a finger. It is a coronavirus test. Mina says that the U.S. should mass-produce these inexpensive and relatively insensitive tests—unlike other methods, they require only a saliva sample—in quantities of tens of millions a day. These tests, which can deliver a result in 15 minutes or less, should then become a ubiquitous part of daily life. Before anyone enters a school or an office, a movie theater or a Walmart, they must take one of these tests. Test negative, and you may enter the public space. Test positive, and you are sent home. In other words: Mina wants to test nearly everyone, nearly every day.
The tests Mina describes already exist: They are sitting in the office of e25 Bio, a small start-up in Cambridge, Massachusetts; half a dozen other companies are working on similar products. But implementing his vision will require changing how we think about tests. These new tests are much less sensitive than the ones we run today, which means that regulations must be relaxed before they can be sold or used. Their closest analogue is rapid dengue-virus tests, used in India, which are manufactured in a quantity of 100 million a year. Mina envisions nearly as many rapid COVID-19 tests being manufactured a day. Only the federal government, acting as customer and controller, can accomplish such a feat.
If it is an audacious plan, it has an audacious payoff. Mina claims that his plan could bring the virus to heel in the U.S. within three weeks. (Other epidemiologists aren’t as sure it would work—at least without serious downsides.) His plan, while costly, is one of the few commensurate in scale to the pandemic: Even if it costs billions of dollars to realize, the U.S. is already losing billions of dollars to the virus every day. More Americans are dying of the coronavirus every month, on average, than died in the deadliest month of World War II. Donald Trump has said that the U.S. is fighting a “war” against an “invisible enemy”; Mina simply asks that the country adopt a wartime economy.
Thousands of students, staff sent home nationwide as COVID snarls school reopenings – ABC
The U.S. attempt to return children to the classroom this fall has turned into a slow-motion train wreck, with at least 2,400 students and staff either infected with COVID-19 or self-isolating because of exposure, and the vast majority of large school districts opting to go online this summer amid rising cases of the virus.
… There is universal agreement that in-person instruction is superior to online classes and particularly vital for at-risk students. But local officials warn of complicating factors: Crowded hallways, opposition to masks, dilapidated buildings with windows sealed shut and reluctant staff.
“There was no way for us to socially distance our children and follow other guidelines” with in-person instruction five days a week, said Helena Miller, chair of the Rock Hill school board in the red state of South Carolina.
Schools in neighboring states this week seemed to make the same point as they struggled to stay open within days or weeks of reopening — many students without masks and walking in crowded hallways. Georgia’s Cherokee County — which was hit the hardest — reported that nearly 1,200 students and staff were self-isolating after known exposures.
Hybrid schooling could be a public health disaster, some doctors warn – The Boston Globe
As communities throughout the state scramble to craft back-to-school plans that prioritize public safety and academics, some officials have lauded hybrid schooling — which includes some variation of both in-school and at-home learning — as a solution that seems to strike an ideal middle ground between the remote-only and full-time camps.
… Call it hopscotch or hybrid or blended learning, but some infectious disease experts call it a potential public health disaster. Alternating schedules could cause children to ebb and flow within an expanded network, transitioning from home to school to child-care centers and thus having a greater risk of exposure or transmission.
“You can see how these got off the ground because it sounds initially like a good idea, but like all things with this virus, you have to think really critically about it,” said Dr. William Hanage, an epidemiologist at Harvard’s T.H. Chan School of Public Health. “When you start to do that, you realize that hybrid schooling actually produces more networks by which the virus can spread.”
… At face value, hybrid plans provide students with some much-desired in-person instruction while lessening the burden on parents who are either working from home themselves or are essential employees who cannot work remotely. Meanwhile, hybrid plans limit class size and, seemingly, the risk to teachers of exposure.
But epidemiologists note that parents who cannot do their jobs remotely and those too busy to oversee at-home learning will still rely on external child-care solutions two to three days a week, further widening the child’s circle of exposure. With fully remote or all in-person learning, children are spending the majority of their time in one or two places with a consistent group. With a hybrid plan, that number balloons to three or more.
Scientists See Signs of Lasting Immunity to Covid-19, Even After Mild Infections – New York Times
Scientists who have been monitoring immune responses to the virus are now starting to see encouraging signs of strong, lasting immunity, even in people who developed only mild symptoms of Covid-19, a flurry of new studies suggests. Disease-fighting antibodies, as well as immune cells called B cells and T cells that are capable of recognizing the virus, appear to persist months after infections have resolved — an encouraging echo of the body’s enduring response to other viruses.
Although researchers cannot forecast how long these immune responses will last, many experts consider the data a welcome indication that the body’s most studious cells are doing their job — and will have a good chance of fending off the coronavirus, faster and more fervently than before, if exposed to it again.
“This is exactly what you would hope for,” said Marion Pepper, an immunologist at the University of Washington and an author on another of the new studies, which is currently under review at the journal Nature. “All the pieces are there to have a totally protective immune response.”
Trump makes call for new White House doctor’s virus advice – AP
President Donald Trump has found a new doctor for his coronavirus task force — and this time there’s no daylight between them.
Trump last week announced that Dr. Scott Atlas, a frequent guest on Fox News Channel, has joined the White House as a pandemic adviser. Atlas, the former chief of neuroradiology at Stanford University Medical Center and a fellow at Stanford’s conservative Hoover Institution, has no expertise in public health or infectious diseases.
But he has long been a critic of coronavirus lockdowns and has campaigned for kids to return to the classroom and for the return of college sports, just like Trump.
U.S. to make coronavirus strain for possible human challenge trials – Reuters
U.S. government scientists have begun efforts to manufacture a strain of the novel coronavirus that could be used in human challenge trials of vaccines, a controversial type of study in which healthy volunteers would be vaccinated and then intentionally infected with the virus, Reuters has learned.
The work is preliminary and such trials would not replace large-scale, Phase 3 trials such as those now under way in the United States testing experimental COVID-19 vaccines from Moderna Inc (MRNA.O) and Pfizer Inc (PFE.N), according to a statement emailed to Reuters by the National Institute of Allergy and Infectious Diseases (NIAID), part of the National Institutes of Health.
U.S. officials organizing the fight against the pandemic have been under pressure from advocacy groups such as 1 Day Sooner and others that see challenge trials as a way to speed up tests of a COVID-19 vaccine. Most vaccine trials rely on inadvertent infection, which can take time to occur.
Some drugmakers, including AstraZeneca (AZN.L) and Johnson & Johnson (JNJ.N), have said they would consider human challenge trials to test COVID-19 vaccines if needed.
Health providers’ scramble for staff and supplies reveals sharp disparities – Politico
Doctors, nurses and caregivers at smaller and poorer hospitals and medical facilities across the country are still struggling to obtain the protective gear, personnel and resources they need to fight the coronavirus … Health care workers at all types of facilities scrambled for scarce masks, gloves and other life-protecting gear at the beginning of the pandemic.
… But now, health care workers say a clear disparity has emerged and persisted. Larger and richer hospitals and practices outbid their smaller peers, sometimes for protective gear, sometimes to fill in staffing gaps. And some of those having the hardest time are precisely where the virus is spreading.
A POLITICO survey of health care workers elicited dozens of stories from the front lines across the country. Reporters did follow up interviews with about a dozen survey respondents, and also interviewed other health care practitioners and policy experts. Some spoke on the condition of anonymity because they feared retribution from employers, as some medical facilities have threatened to fire workers for airing complaints publicly.
CDC asks 4 states and a city to draft coronavirus vaccine distribution plans – Washington Post
Federal health officials are asking four states and one city to draft plans for how they would distribute a coronavirus vaccine when limited doses become available, possibly as early as this fall, officials said.
The Centers for Disease Control and Prevention and the Department of Defense and other agencies began working with officials in California, Florida, Minnesota, North Dakota and Philadelphia this week to develop plans to transport and store vaccine and prioritize which individuals will get the first doses to protect against covid-19, the disease caused by the virus. The proposals will consider each location’s racial and ethnic makeup and population density.
Those plans will be shared with other states to help them with vaccine distribution planning. The discussions with states this week offer some of the first details of the federal government’s plans at a time when information shared by the administration has been limited and often confusing. The United States is planning the largest vaccination campaign ever undertaken, a massive proposition requiring extraordinary coordination, planning and communication.
New research shows that gaiters can protect just as well as other cloth masks. – New York Times
Lightweight neck gaiters, a tube of fabric worn around the neck, have been popular during the pandemic with runners, cyclists and people with beards because they can be pulled up to cover the nose and the mouth and used as a mask.
But in recent days, there has been a backlash against the gaiter. It started after a small study from Duke University showed that a neck gaiter performed poorly when a person wearing a gaiter said the words “Stay healthy, people” five times. During that test, the scientists observed a slight increase in the number of expelled saliva particles when the person wore the gaiter than when the wearer wore nothing at all.
Although the technique the study’s authors used was not a reliable way to measure particles, and their finding was not statistically meaningful, they hypothesized that wearing a neck gaiter might cause more small droplets to spew through the fabric, not fewer.
… Even the study’s authors said their data had been misconstrued. “Our intent was not to say this mask doesn’t work, or never use neck gaiters,” said Martin Fischer, an associate research professor in the department of chemistry at Duke and a co-author of the study.
Dr. Scott Gottlieb: Yale’s new saliva coronavirus test funded by NBA could be widely rolled out – CNBC
- Dr. Scott Gottlieb believes Yale University’s saliva-based coronavirus test is an important development in the United States pandemic response.
- “It’s something that we can roll out on a very wide fashion,” Gottlieb said CNBC on Monday.
- Gottlieb also expects to see “a real explosion” in coronavirus testing opportunities coming onto the market soon.
The following are foreign headlines with hyperlinks to the posts
New Zealand Postpones Elections As It Scrambles To Contain New Coronavirus Outbreak
South Korea Faces New Spike In COVID-19 After Months Of Low Infection Rates
South Korea moves to contain new outbreak, urges people to stay at home
Russia Creating COVID-19 Vaccine for Cats, Minks and Other Animals
Duterte Administration ‘Delighted’ Nearly Half of Filipinos Are Jobless
Italy, Europe’s First COVID-19 Epicenter, Sees New Cases Double in 3 Weeks
Anti-Mask Protests Across Europe as Coronavirus Cases Rise 4 Days in a Row
A South Korean pastor whose church is at the center of a new outbreak has tested positive.
Russia’s vaccine chief claims the West is trying to ‘lure’ away its scientists
Czechs make face masks mandatory again indoors
Bolivia tops 100,000 Covid-19 cases amid protests over election postponement
The following are additional national and state headlines with hyperlinks to the posts
Less Than A Week After Starting Classes, UNC-Chapel Hill Reports 4 COVID-19 Clusters
Significant number of returning Navy midshipmen test positive for coronavirus: report
Like it or not, we’re in the middle of forced education reform
Novavax coronavirus vaccine candidate begins phase two trials
Global Air Travel Down 85 Percent From Same Time Last Year, Experts Say
Why Is There a Pepperoni Shortage?
Trump Reportedly Wants FDA to Approve Plant Extract Oleandrin for COVID-19
300 Pizza Huts are closing after a giant franchisee goes bankrupt
Study finds racial and ethnic disparities in Covid-19 hospitalizations
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
August 2020 Empire State Manufacturing Index Significantly Declined
July 2020 Sea Container Counts Improve And Are Suggesting An Improving Economy
Global Imbalances And The COVID-19 Crisis
Football Fans Think Seasons Shouldn’t Kick Off As Planned
Indigenous Mexicans Turn Inward To Survive COVID-19′ Barricading Villages And Growing Their Own Food
Coronavirus INTERACTIVE Charts
include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus.htm’); ?>
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19. At this point, herd immunity does not look like an option although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a higher death rate.
- There are at least 8 strains of the coronavirus. New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
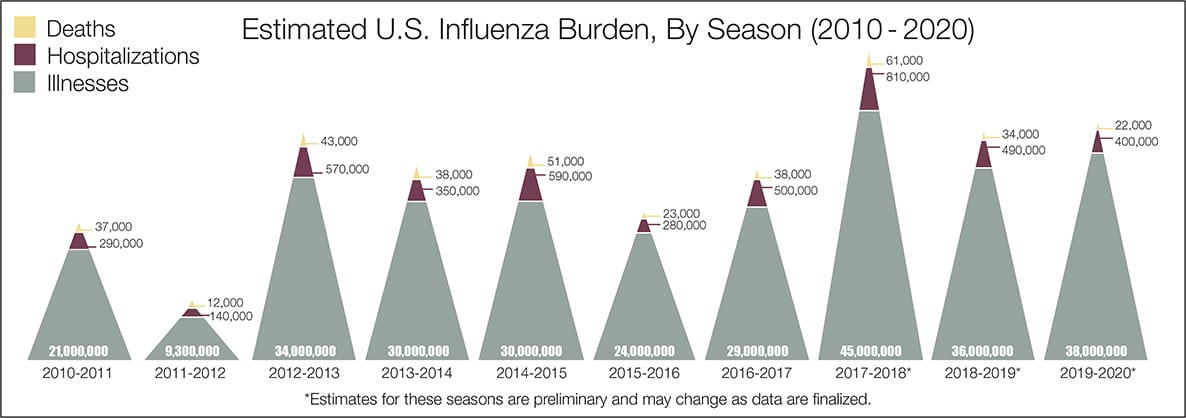
- The real question remains if the U.S. is over-reacting to this virus. The following graphic from the CDC puts the annual flu burden in perspective [click on image to enlarge]. Note that using this data is dangerous as the actual flu cases are estimated and not counted – nobody knows how accurate these guesses are.
What we do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work.
- Do we develop lasting immunity to the coronavirus? Another coronavirus – the simple cold – does not develop long term immunity.
- To what degree do people who never develop symptoms contribute to transmission?
- The US has scaled up coronavirus testing – and the accuracy of the tests has been improving. However, if one loses immunity – the coronavirus testing value is reduced.
- Can children widely spread coronavirus? [current thinking is that they are becoming a major source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- What effect will the weather have? At this point, it does not seem hot weather slows this coronavirus down – and it seems air conditioning contributes to its spread.
- Outdoor activities seem to be a lower risk than indoor activities.
- Can the world really push out an effective vaccine in 12 to 18 months?
- Will other medical treatments for Covid-19 ease symptoms and reduce deaths? So far only one drug (remdesivir) is approved for treatment.
- A current scientific understanding of the way the coronavirus works can be found [here].
Heavy breakouts of coronavirus have hit farm workers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of the respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>





