Written by Steven Hansen
The U.S. and Global new cases 7-day rolling average continues to set new records – and this rolling average in the U.S. new cases are now 10 % higher than one week ago (yesterday it was 12 % which means the rate of acceleration is slowing – the rate of acceleration has been slowing since the end of June). U.S. Death rates due to coronavirus have been holding relatively steady (today deaths were below midrange for values seen in the last few weeks). At the end of this post is a set of interactive graphs and tables for the world and individual states – as well as today’s headlines which include;
- The new case curve is beginning flatten again
- Three simple acts can stop Covid-19 outbreaks
- 138,600 have signed up to test COVID-19 vaccines
- Sweden says people infected with COVID-19 should do contact tracing themselves
- Immuron’s IMM-124E demonstrates antiviral activity against the COVID-19 virus in laboratory studies
- A coronavirus vaccine probably won’t be ready before the end of 2021

My continuing advice is to continue to wash your hands, wear masks, and maintain social distancing. No handwashing, mask, or social distancing will guarantee you do not get infected – but it sure as hell lowers the risk in all situations. In addition, certain activities are believed to carry higher risk – like being inside in air conditioning and removing your mask (such as restaurants, around your children/grandchildren, bars and gyms). It is all about viral load.
The daily number of new cases in the U.S. is remaining stubbornly high, increasing, and the 7-day rolling average continues in record territory.
The following graph showing the 7-day rolling average for new coronavirus cases has been updated through 21 July 2020:

z coronavirus.png
Coronavirus Statistics For 21 July 2020 |
| U.S. Only | Global | U.S Percentage of Total | ||||
| Today*** | Cumulative | Today*** | Cumulative | Today | Cumulative | |
| New Cases | 56,750 | 3,830,000 | 203,467 | 14,680,000 | 27.9% | 26.1% |
| Deaths** | 372 | 140,906 | 4,122 | 610,110 | 9.0% | 23.1% |
| Mortality Rate | 0.7% | 3.7% | 2.0% | 4.2% | ||
total COVID-19 Tests per 1,000 people | 2.32* | 138.17* | ||||
* as of 19 July 2020
** evidently several states included “probable” deaths today in the number
*** red color indicates record number
Coronavirus News You May Have Missed
Three simple acts can stop Covid-19 outbreaks, study finds – CNN
If people washed their hands regularly, wore masks, and kept their social distance from each other, these three simple behaviors could stop most all of the Covid-19 pandemic, even without a vaccine or additional treatments, according to a new study.
The study, published Tuesday in the journal PLoS Medicine, created a new model to look at the spread of the disease and prevention efforts that could help stop it.
The contact rates in the study were based on people’s interaction in the Netherlands, but the model is appropriate for other Western countries, the researchers at the University Medical Center Utrecht said
At a time when some Americans are concerned about the safety of a COVID-19 vaccine, tens of thousands have already volunteered to help bring oneinto existence.
As of Monday , more than 138,600 people had signed up to take part in testing.
“That’s why we’re optimistic that we’re going to be able to get the trials enrolled in an expeditious way. I think we can do what we need to do,” said Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases.
The milestone was reached just a week after the National Institutes of Health launched a clinical trial network for vaccines and other prevention tools to fight the pandemic.
More are still needed, but the initial surge will go a long way toward filling the requirement for at least 30,000 volunteers each for the four companies that plan to launch Phase 3 clinical trials of their potential vaccines by early fall.
Synairgen announces positive results from trial of SNG001 in hospitalised COVID-19 patients – Synairgen
A randomized trial of 101 patients suggests an inhaled form of interferon beta may thwart progression to severe COVID-19
Key findings: The odds of developing severe disease (e.g. requiring ventilation or resulting in death) during the treatment period (day 1 to day 16) were significantly reduced by 79% for patients receiving SNG001 compared to patients who received placebo (OR 0.21 [95% CI 0.04-0.97]; p=0.046). Patients who received SNG001 were more than twice as likely to recover (defined as ‘no limitation of activities’ or ‘no clinical or virological evidence of infection’) over the course of the treatment period compared to those receiving placebo (HR 2.19 [95% CI 1.03-4.69]; p=0.043). Over the treatment period, the measure of breathlessness was markedly reduced in patients who received SNG001 compared to those receiving placebo (p=0.007). Three subjects (6%) died after being randomised to placebo. There were no deaths among subjects treated with SNG001. In the patients with more severe disease at time of admission (i.e. requiring treatment with supplemental oxygen), SNG001 treatment increased the likelihood of hospital discharge during the study, although the difference was not statistically significant (HR 1.72 [95% CI 0.91-3.25]; p=0.096). Median time to discharge was 6 days for patients treated with SNG001 and 9 days for those receiving placebo. Furthermore, patients receiving SNG001 appeared to be more than twice as likely to have recovered by the end of the treatment period (HR 2.60 [95% CI 0.95-7.07]; p=0.062), although this strong trend did not reach statistical significance. However by day 28, patients receiving SNG001 treatment had statistically significantly better odds of recovery (OR 3.86 [95% CI 1.27-11.75]; p=0.017). Interestingly, the efficacy analyses indicate there is no evidence of an association between the SNG001 positive treatment effects and prior duration of COVID-19 symptoms.
How Long Does COVID-19 Immunity Last? – The Atlantic
A new study from King’s College London inspired a raft of headlines suggesting that immunity might vanish in months. The truth is a lot more complicated—and, thankfully, less dire.
But overall, the scientists converged on three reasons to hold out a bit of skepticism about the most apocalyptic headlines.
First, our immune system is a mysterious place, and the KCL study looked at only one part of it. When a new pathogen enters the body, our adaptive immune system calls up a team of B cells, which produce antibodies, and T cells. To oversimplify a bit, the B cells’ antibodies intercept and bind to invading molecules, and the killer T cells seek and destroy infected cells. Evaluating an immune response without accounting for T cells is like inventorying a national air force but leaving out the bomber jets. And, in the case of COVID-19, those bomber jets could make the biggest difference. A growing collection of evidence suggests that T cells provide the strongest and longest-lasting immunity to COVID-19—but this study didn’t measure them at all.
Second, the virologist Shane Crotty told me that while the decline in antibodies was troubling, it was hardly catastrophic. “It’s not unusual to have fading antibody response after several months,” he said. “The drop-off isn’t that surprising. When you look at something like the smallpox vaccine, you see the antibody response is down about 75 percent after six months. But that’s a vaccine that works for decades. We need a study like this to look at COVID patients six months after infection to really know what we’re dealing with.” It’s been six months since the first American COVID-19 patient went to the hospital. Those studies will surely come.
Third, low levels of antibodies can still be enough to knock out COVID-19, because they can prime a larger immune response some time later. “It’s possible that previously-infected people could utilize [immunological memory] responses to produce new antibodies in case they are exposed to SARS-CoV-2 again,” Pamela Bjorkman, a biochemist at the California Institute of Technology, wrote in an email. “So I would not conclude yet that people infected with SARS-CoV-2 are not protected from another infection.”
Sweden says people infected with COVID-19 should do contact tracing themselves – Reuters
Sweden’s health agency said on Monday it was changing its COVID-19 contact-tracing guidelines so that tracing is done to a larger extent by the individuals infected.
The new guidance breaks from a strategy adopted by most countries where authorities trace and notify people who have had close contact with a carrier of the disease.
An agency spokeswoman said it was much better that individuals themselves contact people they may have infected, rather than official tracking units which currently have this responsibility.
The existing system worked well when the number of infections was lower but had become less effective as the number grew, she said.
Unlike most tracing systems, the Swedish system is not anonymous as individuals are expected to deliver the news of their infection to anyone they’ve been in close contact with.
It is not yet clear how this will work in practice or whether authorities will check up on this do-it-yourself arrangement.
Fauci: ‘No End in Sight’ for COVID-19 – MedPage
In contrast to SARS and MERS, COVID-19 has led to almost 15 million infections worldwide and more than 600,000 deaths. The current daily caseload approaches 250,000, and about 5,000 people a day are dying of the infection. Although the pandemic has touched virtually every country in the world, the U.S. has emerged as the global leader in cases (almost 4 million) and deaths (143,500).
Beyond the morbidity and mortality burden, the spectrum of the disease remains striking, said Fauci. In 40%-45% of cases, patients have no symptoms, despite testing positive for exposure to the virus. From there, symptoms run the gamut from mild (uncomplicated upper respiratory tract infection) to critical illness (acute respiratory distress, septic shock, multiorgan system failure). Patients who are asymptomatic or have mild/moderate symptoms account for about 80% of all cases.
The large percentage of patients with asymptomatic infection confounds efforts to determine the true infection-related mortality, he said. A widely cited study from China showed a case-fatality rate of 2.3% in 44,672 infected patients. “If you count all of the people who are asymptomatic, it’s likely that the total fatality rate is around 1% or less.”
Immuron Reports Neutralizing Activity Against SARS-CoV-2 Key Points – Seeking Alpha
- Immuron’s IMM-124E used to manufacture Travelan® and Protectyn® demonstrates antiviral activity against the COVID-19 virus in laboratory studies
- Immuron’s technology platform offers a potential new oral therapeutic approach to target SARS-CoV-2 in the GI Tract
Said Dr Jerry Kanellos, CEO of Immuron Limited.
“We know that SARS-CoV-2 causes an influenza-like disease that is primarily thought to infect the lungs with transmission through the respiratory route ranging from mild respiratory symptoms to severe lung injury, multiorgan failure, and death. Respiratory symptoms have dominated the clinical focus, however gastrointestinal symptoms such as diarrhea, vomiting, and abdominal pain are also observed in a growing subset of patients often presenting with no respiratory symptoms. In the United States the Centers for Disease Control and Prevention recently updated the symptoms of coronavirus to include diarrhea. This growing clinical evidence suggests that the Gastrointestinal tract may present another viral target organ. The virus RNA has been detected in anal swabs of patients even after nasopharyngeal testing has turned negative, and cells in the inner-gut lining express high amounts of the angiotensin-converting enzyme 2 (ACE2) receptor that SARS-CoV-2 uses to gain entry to cells implying the potential for gastrointestinal infection and a fecal-oral transmission route. If fecal-oral transmission is a significant factor in the pandemic then the consequences for an oral therapeutic would be significant, however the research is still inconclusive. The preliminary data set we have generated potentially offers a new oral therapeutic approach to target and directly inhibit the virus in the Gastrointestinal tract and warrants further evaluation to identify the inhibitory substances in our products. The company has filed a provisional patent application in respect of the findings.”
U.S. charges two Chinese nationals in coronavirus vaccine hacking scheme, other crimes – CNBC
- The Department of Justice accused two Chinese nationals, who it said were working on behalf of the Chinese government, of stealing trade secrets and hacking into computer systems of firms working on the Covid-19 vaccine.
- According to the 11-count indictment, Li Xiaoyu, 34, and Dong Jiazhi, 33, conducted a global hacking campaign for more than a decade.
- More recently, the defendants probed for vulnerabilities in computer networks of companies developing Covid-19 vaccines, testing technology, and treatments,” a DOJ statement said.
Airline CEOs urge Trump administration, EU for Covid-19 passenger testing – Reuters
The CEOs of major U.S. airlines are set to hold a meeting Friday to discuss several coronavirus-related travel issues, including a push to convince the federal government to mandate temperature checks for passengers, three people briefed on the matter said.
Several airline CEOs are urging the Trump administration and the European Commission to back Covid-19 tests for passengers to help lift bans on many potential travelers between the U.S. and Europe.
Government travel restrictions bar most would-be travelers from entering either region, depriving airlines of revenue for what were some of their most important routes. The CEOs called for a pilot testing program to “build confidence and safely restore passenger travel between the U.S. and Europe.”
The C.D.C. says the number of people infected ‘far exceeds the number of reported cases’ in parts of the U.S. – New York Times
The number of people infected with the coronavirus in different parts of the United States was anywhere from two to 13 times higher than the reported rates for those regions, according to data released Tuesday by the Centers for Disease Control and Prevention.
The findings suggest that large numbers of people who did not have symptoms or did not seek medical care may have kept the virus circulating in their communities. The study is the largest of its kind to date, although some early data was released last month.
“These data continue to show that the number of people who have been infected with the virus that causes Covid-19 far exceeds the number of reported cases,” Dr. Fiona Havers, the C.D.C. researcher who led the study, said in an email. “Many of these people likely had no symptoms or mild illness and may have had no idea that they were infected.”
Pharmaceutical executives tell Congress a vaccine might be ready within six months. – New York Times
Executives from four companies in the race to produce a coronavirus vaccine told lawmakers on Tuesday that they are optimistic their products could be ready by the end of 2020 or the beginning of 2021. All four companies — AstraZeneca, Johnson & Johnson, Moderna Therapeutics and Pfizer — are testing proprietary vaccines in various phases of human clinical trials.
“We would hope in the fall or towards the end of the year we have data that we could submit to the FDA for them to make a determination on whether to approve it,” said Dr. Stephen Hoge, the president of Moderna. He added, “We would also hope at that point to have millions of doses of vaccine available for deployment.”
Three of the firms have received federal government funding for their vaccine development efforts. AstraZeneca and Johnson & Johnson, two of the recipients, pledged to the lawmakers that they would produce hundreds of millions of doses of their vaccines at no profit to themselves. Moderna, however, which has received $483 million from the government for its coronavirus research, said it would not be selling its vaccine at cost.
A coronavirus vaccine probably won’t be ready before the end of 2021, according to a Swiss pharmaceutical giant – Business Insider
- A coronavirus vaccine will “most likely” not be ready before the end of 2021, according to the head of the world’s second-largest pharmaceutical company.
- “I’m afraid that the most likely scenario is that we will not have a vaccine before the end of next year,” Severin Schwan, the CEO of Roche, said on a call with reporters on Wednesday.
- Schwan said an antibody test — which can determine whether someone has had COVID-19 and could be launched as early as May — would instead be the key to allowing people to return to normal life.
- Some leading researchers are more optimistic that a vaccine could be developed and rolled out this year.
The following are foreign headlines with hyperlinks to the posts
Coronavirus threatens to disrupt South Korea-US military exercises
Brazil Tops 80,000 COVID-19 Deaths As 2 Government Ministers Test Positive For Virus
EU Agrees To $858 Billion In Grants, Loans To Bail Out Pandemic-Battered Economies
Coronavirus: No ‘foolproof’ prevention measures as Hong Kong sees 2 more deaths and 61 new cases
COVID-19: Zimbabwe imposes dusk-to-dawn curfew
Austria reintroducing face mask requirement in supermarkets, banks
The following are additional national and state headlines with hyperlinks to the posts
California reports nearly 12,000 COVID cases, biggest increase since pandemic started
Dr. Anthony Fauci To Throw First Pitch For Washington Nationals’ Season Opener
South Carolina Hospitals Face Down COVID Surge
Record Low Mortgage Rates Put More Cash In Pockets, But May Not Boost Economy Much
Florida Teachers Sue To Block School Coronavirus Reopening Mandate
Visitors from 31 states now required to quarantine when visiting New York, New Jersey, Connecticut
New York City spent $52 million on coronavirus hospital that served 79 patients
Men’s Wearhouse owner Tailored Brands plans to shut 500 stores, cut 20% of corporate workforce
More tech layoffs: Sunnyvale’s LinkedIn to cut 960, 6 percent of its workforce
Amazon officially delays Prime Day, but hasn’t set a new date
500 women at Texas federal prison test positive for COVID-19
White House says Trump gets tested ‘multiple times a day’ for coronavirus
States with the Fewest Coronavirus Restrictions
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
June 2020 CFNAI Super Index Moving Average Index Suggests Economic Growth Again Improved
May 2020 CoreLogic Single-Family Rent Index Significantly Declines
News Cuts Up 170% Over 2019, Worst Year For Newsrooms On Record
Infographic Of The Day: Stay Productive When Working From Home
Protracted G7 Contraction – Or Multiyear Global Depression
Chinese Economy Rebounds From COVID-19 Setback
Video: An Infectious Disease Expert Explains The Results From Moderna’s Latest Vaccine Trials
Average Gasoline Prices for Week Ending 20 July 2020 Down $0.56 From A Year Ago
Coronavirus INTERACTIVE Charts
include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus.htm’); ?>
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19. At this point, herd immunity does not look like an option.
- Older population countries will have a higher death rate.
- There are at least 8 strains of the coronavirus. New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
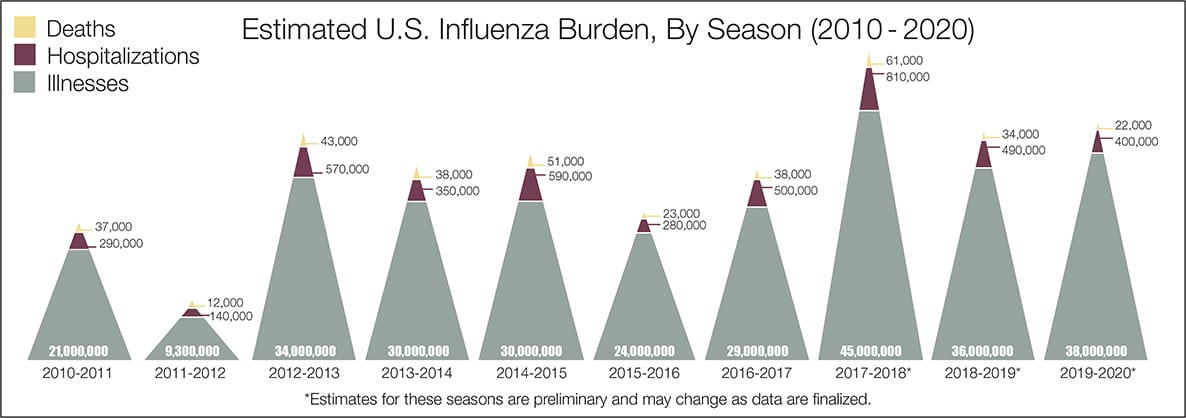
- The real question remains if the U.S. is over-reacting to this virus. The following graphic from the CDC puts the annual flu burden in perspective [click on image to enlarge]. Note that using this data is dangerous as the actual flu cases are estimated and not counted – nobody knows how accurate these guesses are.
What we do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work.
- Do we develop lasting immunity to the coronavirus? Another coronavirus – the simple cold – does not develop long term immunity.
- To what degree do people who never develop symptoms contribute to transmission?
- The US has scaled up coronavirus testing – and the accuracy of the tests has been improving. However, if one loses immunity – the coronavirus testing value is reduced.
- Can children widely spread coronavirus?
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- What effect will the weather have? At this point, it does not seem hot weather slows this coronavirus down – and it seems air conditioning contributes to its spread.
- Outdoor activities seem to be a lower risk than indoor activities.
- Can the world really push out an effective vaccine in 12 to 18 months?
- Will other medical treatments for Covid-19 ease symptoms and reduce deaths? So far only one drug (remdesivir) is approved for treatment.
- A current scientific understanding of the way the coronavirus works can be found [here].
Heavy breakouts of coronavirus have hit farmworkers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of the respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>





