
Written by Steven Hansen
The U.S. new cases 7-day rolling average are 14.6 % LOWER than the 7-day rolling average one week ago. U.S. hospitalizations due to COVID-19 are now 11.0 % LOWER than the rolling average one week ago. U.S. deaths due to coronavirus are now 1.8 % HIGHER than the rolling average one week ago. Today’s posts include:
- U.S. Coronavirus New Cases are 138,746
- U.S. Coronavirus hospitalizations are at 97,561
- U.S. Coronavirus deaths are at an elevated 2,664
- U.S. Coronavirus immunizations have been administered to 9.4 % of the population
- The 7-day rolling average rate of growth of the pandemic shows new cases improved, hospitalizations improved, and deaths improved
- Current charts are showing a “holiday” peak is behind us – hopefully, this improving trend will remain in play even with the new strains
- Pfizer and Moderna did their clinical trials before the variant strains became very apparent. Johnson & Johnson was testing its vaccine not only against the standard strain but they had the variants.
- ‘COVID Tongue’ May Be a Symptom
- Diabetes treatment may protect against COVID-19 mortality
- Everything you need to know about double-masking
- The finding in Minnesota last week of the nation’s first COVID-19 infection from a more contagious Brazilian variant is raising concerns that pandemic cases could accelerate
- The U.S. has Covid-19 vaccines but few treatments. What happened?
- Dubai forms Vaccine Logistics Alliance to expedite distribution of 2 billion Covid-19 vaccines

The recent worsening of the trendlines for new cases is behind us which was attributed to going back to college/university, cooler weather causing more indoor activities, mutation of the virus, fatigue from wearing masks / social distancing, holiday activities, and some loosening of regulations designed to slow the coronavirus spread.
My continuing advice is to continue to wash your hands (especially after using the toilet as COVID first sheds in your stool), putting down the toilet seat (as flushing the toilet releases a plume), wear masks, avoid crowds, and maintain social distancing. No handwashing, mask, or social distancing will guarantee you do not get infected – but it sure as hell lowers the risk in all situations – and the evidence to-date shows a lower severity of COVID-19. In addition, certain activities are believed to carry a higher risk – like being inside in air conditioning and removing your mask (such as restaurants, around your children/grandchildren, bars, and gyms). It is all about viral load – and outdoor activities are generally safe if you can maintain social distance. Finally, studies show eating right (making sure you are supporting your immune system) and adequate sleep increase your ability to fight off COVID.
include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus1.htm’); ?>
Hospitalizations (grey line) and Mortality (green line)
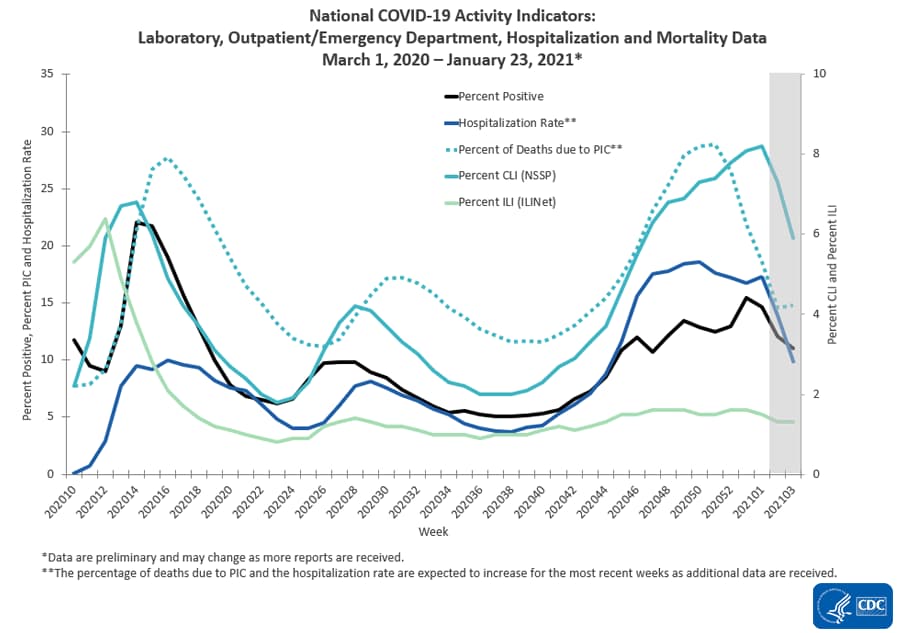
source: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html
Hospitalizations Are The Only Accurate Gauge As Reporting Is Not Affected By Holidays
The 4 day Thanksgiving holiday period put the first wobble in the trends. Over weekends and holidays, the number of new cases and deaths decline. Over weekends, this is not a problem for week-over-week rolling averages as weekends are compared against the previous weekend. But when a holiday falls within a working week, a non-working day is compared to a working day which causes havok in the trends.
However, hospitalizations historically appear to be little affected by weekends or holidays – the daily counts do not vary significantly from day-to-day.
The hospitalization growth rate trend is improving.

For the Thanksgiving and the end of the year holiday period – roughly, it seems each appears to have added around 5 % to the rate of growth of new cases, hospitalizations, and deaths.
Historically, hospitalization growth follows new case growth by one to two weeks.
As an analyst, I use the rate of growth to determine the trend. But, the size of the pandemic is growing in terms of real numbers – and if the rate of growth does not become negative – the pandemic will overwhelm all resources.
The graph below shows the rate of growth relative to the growth a week earlier updated through today [note that negative numbers mean the rolling averages are LOWER than the rolling averages one week ago]. As one can see, the rate of growth for new cases peaked in early December 2020 for Thanksgiving, and early January 2021 for end of year holidays – and the rate of growth is now contracting.

In the scheme of things, new cases decline first, followed by hospitalizations, and then deaths.
It is up to each of our readers to protect themselves and others by washing your hands, wearing a mask, avoiding crowds, and maintaining social distancing.
Will The New Variants Cause The Next Spike?
Maybe and maybe not. It all depends on vaccinations:
- the more people that are vaccinated reduces the pool of people that can be infected. Today we have removed over 9 % of the population from being infected which theoretically should reduce the infection rate by 9 % [it is unstudied whether the vaccines prevent a vaccinated person from being a carrier of the virus even though showing no signs]. If the vaccines are shown to stop transmission, then in theory it would reduce the infection rate by double the percent vaccinated [in this case you prevent your own infection and do not pass it along to another].
- it is also unknown what the effective rate of the current vaccines is against mutations that seem to appear almost daily. As an example, if the effective rate drops to 60%, it means the 9 % reduction in the infection rate discussed above is almost cut in half. The South African and Brazilian variant is somewhat immune to the current vaccines.
- The pandemic should be over immediately if everyone could be vaccinated today. The problem is that every day brings a new mutation (which would not appear if the pandemic was stopped). The longer the immunization process takes – the more ineffective the vaccine will become.
- It is not clear whether the vaccine prevents those vaccinated from spreading the virus. It seems to be well documented that it normally stops the virus from taking hold and when it does not – the infection is mild.
Coronavirus News You May Have Missed
Econintersect published two summary articles today for coronavirus news this past week:
Lower efficacy vaccines are still worthwhile, experts say. – New York Times
At first glance, the results reported on Friday from the long-awaited trial of Johnson & Johnson’s Covid-19 vaccine might have seemed disappointing. Its overall efficacy – the ability to prevent moderate and severe disease – was reported at 72 percent in the United States, 66 percent in Latin American countries and 57 percent in South Africa.
Those figures appear far below the high bar set by Pfizer-BioNTech and Moderna, the first two vaccines authorized for emergency use in the United States, which reported overall efficacy from 94 to 95 percent.
But Dr. Anthony S. Fauci, the nation’s leading infectious disease expert, said that the more crucial measure was the ability to prevent severe disease, which translates to keeping people out of the hospital and preventing deaths. And that result, for Johnson & Johnson, was 85 percent in all of the countries where it was tested, including South Africa, where a rapidly spreading variant of the virus had shown some ability to elude vaccines.
More important than preventing “some aches and a sore throat,” Dr. Fauci said, is to fend off severe disease, especially in people with underlying conditions and in older adults, who are more likely to become seriously ill and to die from Covid-19.
Researchers warn that trying to compare effectiveness between new studies and earlier ones may be misleading, because the virus is evolving quickly and to some extent the trials have studied different pathogens.
“You have to recognize that Pfizer and Moderna had an advantage,” Dr. William Schaffner, an infectious disease expert at Vanderbilt University, said in an interview. “They did their clinical trials before the variant strains became very apparent. Johnson & Johnson was testing its vaccine not only against the standard strain but they had the variants.”
Everything you need to know about double-masking – USA Today
The Centers for Disease Control and Prevention (CDC) has been recommending people wear face masks since early April. Because of the shortage of N95 masks, cloth face masks have become the norm, with many options available from homemade ones on Etsy to masks from large retailers, including our favorite the Athleta Non Medical Mask.
I’ve been evaluating many of these cloth options since they first hit the market. Before joining Reviewed, I spent most of my career in apparel and textiles. Most recently I was at Nike, where I evaluated the quality of materials and determined if they were fit for use for apparel products. I’m definitely a materials nerd. I’ve rigorously tested and worn dozens of masks, and evaluated them for quality, comfort and fit to find the best ones. And the need for cloth face masks has not gone away.
… Whether you wear one face mask or more, it should be a quality face mask. I’ve previously written about what to look for in a quality mask and some of the most important things to look for are multiple layers, tightly woven fabric, and a snug fit to the face. We love Athleta’s Everyday Non Medical Mask, which won an Editor’s Choice award for Best Overall. This mask strikes a nice balance between protection and breathability. It has triple-layered woven fabric, a bendable nose piece, and adjustable ear loops which help with a snug fit to the face.
Are two masks better than one?
According to Dr. Anthony Fauci, the director of the National Institute of Allergy and Infectious Diseases, wearing two masks is common sense. Fauci told NBC News’ TODAY “If you have a physical covering with one layer, you put another layer on, it just makes common sense that it likely would be more effective.”
Studies have found that multiple layers of fabric in a mask increase filtration effectiveness from virus particles. Following that logic, By double-masking, a person increases the number of layers of fabric protecting their face, thereby upping the level of filtration.
From my years of working with fabrics, this concept makes sense. Woven fabric is essentially a mesh grid made of threads. The more these grids layer on top of each other, the more likely holes are covered, which then creates more areas for respiratory particles to get blocked or trapped before they make it to your face.
Should I wear two masks?
The CDC has not issued official guidance on double-masking, however, the evidence suggests two masks are likely more effective than a single mask. In situations where you are not able to social distance, you may want to double up by wearing a cloth mask over a surgical mask or two cloth masks.
In the early days of the pandemic, medical workers were double-masking to try to extend the life of scarce N95 masks, which continue to be in short supply.
One drawback of wearing two masks is that the multiple layers of material could make it harder to breathe. If you already have trouble breathing while wearing one mask, adding another may not be the best option. The CDC notes wearing one mask is better than not wearing any face covering.
‘COVID Tongue’ May Be a Symptom, Professor Says – Medscape
A professor in the United Kingdom says he’s finding more COVID-19 patients reporting oral problems, such as tongue discoloration and enlargement.
“Seeing increasing numbers of COVID tongues and strange mouth ulcers. If you have a strange symptom or even just headache and fatigue stay at home!” tweeted Tim Spector, a professor of genetic epidemiology at King’s College London, who included one of the many tongue photos he receives daily.
“My mail is full of tongues each morning from people who had tongue problems that coincided with COVID symptoms like fever and fatigue – but baffled doctors. Happy to share so we all become experts … ,” he tweeted.
He said 35% of people exhibit non-classic symptoms of COVID in the first 3 days, such as “skin rashes, COVID toes and the 20+ symptoms of COVID that go ignored.”
The CDC does not include swollen or discolored tongues as symptoms of COVID-19, but the list of symptoms has grown since the pandemic began.
“This is kind of in tune with all of the things about COVID. When it burst upon the scene, as I like to say figuratively, we opened up our medical textbooks to COVID and there were only blank pages,” said William Schaffner, MD, professor of infectious diseases at Vanderbilt University School of Medicine in Nashville, according to NBC News .
“So since then, we’ve been filling in the blank pages lickety-split and it may well be that this is part of the clinical syndrome that some patients have.”
NBC News said a study of Spanish COVID patients found a little more than 10% had some sort of oral problem, such as swollen tongue or mouth ulcers.
Dubai forms Vaccine Logistics Alliance to expedite distribution of 2 billion Covid-19 vaccines – CNN
United Arab Emirates announced it will launch the Vaccine Logistics Alliance to “equitably distribute” 2 billion doses of Covid-19 vaccines in 2021, according to a statement released by the Government of Dubai Media Office.
The alliance will bring together Emirates airline, logistics company DP World, Dubai Airports, pharmaceutical manufacturer, and other government agencies to transport the vaccines.
“The distribution will particularly focus on emerging markets, where populations have been hard-hit by the pandemic, and pharmaceutical transport and logistics are challenging,” according to the statement.
In December the People’s Vaccine Alliance said rich countries had bought enough Covid-19 vaccine doses to immunize their populations three times over, but that developing countries are being left behind in the global sprint to end the pandemic.
In 67 poorer nations, just one in 10 people can hope to receive a vaccine by the end of 2021, the international vaccine watchdog added.
The group urged pharmaceutical companies to share their technology and intellectual property with the World Health Organization and urged governments to commit to sending vaccines to the developing world, in order to close the economic disparity between nations as they look to emerge from the devastating Covid-19 crisis.
Diabetes treatment may protect against COVID-19 mortality – Medical News Today
- Upon analyzing data from a diverse patient population, the researchers found that individuals who had been taking metformin, a drug for type 2 diabetes, were less likely to die of COVID-19 than those not on metformin.
- Their study also highlighted the fact that Black people made up a disproportionate number of those who tested positive for COVID-19.
- According to the researchers, this disparity is likely due to socioeconomic factors, lack of access to healthcare, and a higher risk of exposure to SARS-CoV-2 among Black populations.
Dangerous new coronavirus strains may incubate in COVID-19’s sickest – Yahoo
Among the 100 million people around the world who have battled coronavirus infections, scientists are turning to the case of a 45-year-old COVID-19 patient in Boston to understand how the virus is able to outwit humans.
During his 154-day illness – one of the longest on record – the patient’s body became a crucible of riotous viral mutation. He offered the world one of the first sightings of a key mutation in the virus’ spike protein that set off alarm bells when it was later found in strains in the United Kingdom, South Africa and Brazil.
In the U.K. strain, the genetic change known as N501Y is thought to help enhance the virus’ transmissibility by about 50%. In the South Africa strain, it may reduce the effectiveness of COVID-19 vaccines and treatments. Tests of its effect on the Brazil variant are still in progress.
The Boston patient is now being viewed as an important harbinger of the coronavirus’ ability to spin off new and more dangerous versions of itself. Though he died over the summer, the medical file he left behind is helping experts anticipate the emergence of new strains by focusing on the role of a growing population of patients with compromised immune systems who battle the virus for months.
Among the sickest of COVID-19 patients, this population of “long haulers” appears to play a key role in incubating new variants of the coronavirus, some of which could change the trajectory of the pandemic.
The mutations that arose from this single patient are “a microcosm of the viral evolution we’re seeing globally,” said Dr. Jonathan Z. Li, an infectious-disease specialist at Brigham and Women’s Hospital in Boston who treated him. “He showed us what could happen” when a germ with a knack for genetic shape-shifting stumbles upon conditions that reward it for doing so.
Indeed, situations in which patients can’t clear a viral infection are “the worst possible scenario for developing mutations,” said Dr. Bruce Walker, an immunologist and founding director of the Ragon Institute in Boston.
Coronavirus variant finding in Minnesota raises troubling questions – Star Tribune
The finding in Minnesota last week of the nation’s first COVID-19 infection from a more contagious Brazilian variant is raising concerns that pandemic cases could accelerate, although more information is needed on the exact nature of the threat.
As with variants that have emerged in the United Kingdom and South Africa, scientists believe the strain spreads more easily and quickly than others, potentially sickening more people.
But health officials don’t know for sure if it’s spreading in Minnesota. The state Department of Health said last week that it identified the strain in a specimen from a resident who recently traveled to the South American nation. It’s also not clear the extent to which immune system protection that’s been stimulated by vaccines or a previous SARS-CoV-2 infection will work against the Brazil variant.
Worries over the variants come amid otherwise encouraging signs about the pandemic in Minnesota, with thousands of residents being vaccinated each day and a recent decline in new cases.
“We are in a very, very difficult period,” said William Hanage, an epidemiologist with the Harvard T.H. Chan School of Public Health. “The variants of concern are … serious causes of concern, but we don’t know enough about them at the moment to be able to be definitive.
“And this is happening at a time when vaccines are beginning to become available and people are starting to feel like they’re going to be able to relax. That’s dangerous for a lot of reasons.”
The Most Worrying Mutations in Five Emerging Coronavirus Variants – Scientific American
Names: 20A.EU1, B.1.177
Notable mutation: A222VThe 20A.EU1 variant, first identified in Spain, contains a mutation called A222V on the viral spike protein. The spike is a component of SARS-CoV-2 that binds to a receptor on human cells called ACE2, and this attachment helps the virus get inside those cells and infect them. The spike protein is also the part of the pathogen that is targeted by human antibodies when they fight back against the infection. In lab tests, human antibodies were slightly less effective at neutralizing viruses with the A222V mutation. Over the course of several months, the 20A.EU1 variant became the dominant one in Europe. Epidemiologists never saw any evidence that it was more transmissible than the original, however. Researchers believe that when Europe began lifting travel restrictions last summer, the variant that was dominant in Spain spread across the continent.
Names: 20I/501Y.V1, VOC 202012/01, B.1.1.7
Notable mutation: N501YScientists in the U.K. had been watching the B.1.1.7 variant for some time before announcing in December that it might be at least 50 percent more transmissible than the original form. That announcement was based on epidemiological data that showed the virus rapidly spreading throughout the nation. And it led to international travel bans and stronger lockdown measures in the U.K.
The B.1.1.7 variant contains 17 mutations, including several in the spike protein. One of them, N501Y, has been found to help the virus bind more tightly to the ACE2 cellular receptor. It is unclear, however, whether the variant’s enhanced contagiousness comes from N501Y alone or also involves some combination of other spike protein mutations.
Despite initial concerns, there has been no real evidence that the variant is more infectious in children than the original, says University of Cambridge microbiologist Sharon Peacock, who is executive director of the COVID-19 Genomics UK (COG-UK) Consortium, a group that analyzes genetic changes to the virus. Both Pfizer and Moderna believe that their COVID-19 vaccines will still work against B.1.1.7. Recent data from the U.K. hint that the variant may be more lethal than the original, but the analyses are preliminary.
B.1.1.7 does stand out because it accumulated so many mutations, apparently all at once. Lauring and others suspect that these mutations may have arisen within one immunocompromised patient who was infected for a long time because that person was unable to fight off the virus. It is likely that only a few of these changes gave the variant an evolutionary advantage and allowed it to quickly spread around the U.K., says Scott Weaver, a microbiologist at the University of Texas Medical Branch at Galveston. The others were simply along for the ride.
Names: 20H/501Y.V2, B.1.351
Notable mutations: E484K, N501Y, K417NThe B.1.351 variant appeared around the same time as B.1.1.7, and it spread quickly in South Africa to become the dominant version in that country. Like its European counterpart, B.1.351 contains the N501Y mutation, although evidence seems to suggest the two variants arose independently. But scientists are more concerned about another mutation called E484K that appears in the South African version. The genetic change may help the virus evade the immune system and vaccines.
Using yeast cells, evolutionary and computational biologist Jesse Bloom of the Fred Hutchinson Cancer Research Center in Seattle and his lab created a series of spike proteins with almost all of the more than 3,800 possible protein component changes that could be driven by genetic mutations. Then the scientists tested how well or poorly human antibodies bound to each altered spike. They found that E484K-as well as similar mutations at that particular spot in the protein-made it as much as 10 times more difficult for antibodies to bind to the spike in some people. Bloom’s lab also found that some antibody cocktails, such as one currently being tested by the drug and biotech companies Regeneron and Eli Lilly, may be less effective against mutations present in the B.1.351 variant.
Late this month researchers in South Africa released a preprint study (research that has not yet been peer-reviewed) showing that an antibody-containing serum from COVID patients was considerably less effective at neutralizing this variant. And in another preliminary preprint posted on January 26, scientists reported they put B.1.351 into serum taken from people who had been vaccinated with either the Pfizer or Moderna vaccine. They found antibodies in that serum showed reduced neutralizing activity against the mutant, compared with their activity against the original virus.
Antibodies in test tubes are not the same thing as vaccines in real people, however. Both vaccines produce so many antibodies that a drop in activity could still leave enough of them to neutralize the virus. The vaccines also stimulate other protective components of the immune system. Still, Moderna has begun work on a booster shot specific to new variants.
Names: B.1.1.28, VOC202101/02, 20J/501Y.V3, P.1
Notable mutations: E484K, K417N/T, N501YNames: VUI202101/01, P.2
Notable mutation: E484KIn January researchers reported they had detected two new variants in Brazil, both descendants of a somewhat older common ancestor variant. Although they share mutations with other newly discovered versions, they appear to have arisen independently of those variants.
Of the two, researchers are currently more concerned about P.1. That variant contains more mutations than P.2 (though both have E484K), and it has already been seen in Japan and other countries. Although it is possible that P.1 accumulated its mutations in an immunocompromised individual, genetics researcher Emma Hodcroft of the University of Bern in Switzerland says that it might be more difficult to pinpoint the time and place when this variant first arose because Brazil does not sequence nearly as many viral samples as the U.K.
Hodcroft points out that both Brazil and South Africa had large COVID outbreaks in 2020. With so many infected people creating antibodies against the virus, a version that could evade the immune system and reinfect a person who had recovered might have a strong advantage and then become more widespread in a population.
VIRAL SPREAD AND CHANGE
Although the seemingly sudden emergence of several spike protein variants is reason for concern, researchers say there is no evidence that the virus has changed in a fundamental way that lets it mutate more rapidly. What is most likely, Lauring says, is that the sheer number of COVID cases worldwide is allowing the virus numerous opportunities to change a little bit. Each infected person is, essentially, a chance for SARS-CoV-2 to reinvent itself. “Some of it is evolution, but a lot of it is epidemiology,” Lauring says. Overall, “the virus is getting better at being a virus.”
The U.S. has Covid-19 vaccines but few treatments. What happened? – New York Times
Nearly a year into the pandemic, as thousands of patients are dying every day in the United States and widespread vaccination is still months away, doctors have precious few drugs to fight the virus.
A handful of therapies – remdesivir, monoclonal antibodies and the steroid dexamethasone – have improved the care of Covid patients, putting doctors in a better position than they were when the virus surged last spring. But these drugs are not cure-alls and they’re not for everyone, and efforts to repurpose other drugs, or discover new ones, have not had much success.
The government poured $18.5 billion into vaccines, a strategy that resulted in at least five effective products at record-shattering speed. But its investment in drugs was far smaller, about $8.2 billion, most of which went to just a few candidates, such as monoclonal antibodies. Studies of other drugs were poorly organized.
The result was that many promising drugs that could stop the disease early, called antivirals, were neglected. Their trials have stalled because researchers could not find either enough funding or enough patients to participate.
At the same time, a few drugs have received sustained investment despite disappointing results. There is now a wealth of evidence that the malaria drugs hydroxychloroquine and chloroquine do not work against Covid. And yet there are still 179 clinical trials with 169,370 patients in which at least some are receiving the drugs, according to the Covid Registry of Off-label & New Agents at the University of Pennsylvania. And the federal government funneled tens of millions of dollars into an expanded access program for convalescent plasma, infusing almost 100,000 patients before there was any robust evidence that it worked. In January, those trials revealed that, at least for hospitalized patients, it doesn’t.
The lack of centralized coordination meant that many trials for Covid antivirals were doomed from the start – too small and poorly designed to provide useful data, according to Dr. Janet Woodcock, the acting commissioner of the Food and Drug Administration. If the government had instead set up an organized network of hospitals to carry out large trials and quickly share data, researchers would have many more answers now.
The following are foreign headlines with hyperlinks to the posts
EU Reverses Move To Restrict Export Of COVID-19 Vaccines To Northern Ireland
Nine children with symptoms of Covid-19 have died in the Yanomami Indigenous Territory in the Amazonas state of Brazil
South Korea extends social distancing measures for Lunar New Year holiday
Western Australia locks down three regions after hotel security guard tests positive
Australia reopens travel bubble for people traveling from New Zealand
WHO team goes to wholesale market in Wuhan during investigation of Covid-19 origin
Germany is already ordering Covid-19 vaccines for 2022
Two-month-old infant with health problems dies after contracting coronavirus
The following additional national and state headlines with hyperlinks to the posts
COVID-19 halts America’s homeless count
It’s not just you. There is a Grape-Nuts shortage.
Los Angeles vaccination site temporarily shut down after protestors block entrance [protestors were holding posters with the words, “99.96% survival rate” and “End the Lockdown” as well as other paraphernalia that appeared to denounce the pandemic’s existence and coronavirus vaccinations.]
Democratic lawmaker vaccinated for COVID-19 tests positive
Connecticut health system cancels vaccination appointments due to shortages
Fourth COVID Case Reported at Iowa Capitol Where Masks Are Not Required
Why Getting Third Stimulus Check Not Guaranteed Even if You Got First Two
How one California college is trying to shield its city from the virus.
The virus’s path through Los Angeles is unequal.
The US has administered nearly 30M doses of Covid-19 vaccine
US hospitalizations fall below 100,000 for the first time in nearly two months
The other rebellion: Dozens of Michigan restaurants defy state coronavirus order
At Louisiana nursing homes, testing lags likely increased the deadly coronavirus toll
We’re selling the coronavirus vaccine short
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
Can Employers Mandate The COVID-19 Vaccine?
What The Continued Global Uncertainty Means For You
Coronavirus Disease Weekly News 31January 2021
Coronavirus Economic Weekly News 31January 2021
Warning to Readers
The amount of politically biased articles on the internet continues to increase. And studies and opinions of the experts continue to contradict other studies and expert opinions. Honestly, it is difficult to believe anything anymore. A study usually cannot establish cause and effect – but only correlation. Be very careful what you believe about this pandemic.

I assemble this coronavirus update daily – sifting through the posts on the internet. I try to avoid politically slanted posts (mostly from CNN, New York Times, and the Washington Post) and can usually find unslanted posts on that subject from other sources on the internet. I wait to publish posts on subjects that I cannot validate across several sources. But after all this extra work, I do not know if I have conveyed the REAL facts. It is my job to provide information so that you have the facts necessary – and then it is up to readers to draw conclusions.
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19 when recovering from COVID-19. Herd immunity does not look like an option without immunization although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a significantly higher death rate as there is relatively few hospitalizations and deaths in younger age groups..
- There are at least 8 strains of the coronavirus. New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
What we do or do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work. Unfortunately, early in the pandemic, many health experts – in the U.S. and around the world – decided that the public could not be trusted to hear the truth about masks. Instead, the experts spread a misleading message, discouraging the use of masks.
- Current thinking is that we develop 5 months of immunity from further COVID infection.
- The Moderna and Pfizer vaccines have an effectiveness rate of about 95 percent after two doses. That is on par with the vaccines for chickenpox and measles. The 95 percent number understates the effectivenessas it counts anyone who came down with a mild case of Covid-19 as a failure. But turning Covid into a typical flu – as the vaccines evidently did for most of the remaining 5 percent – is actually a success. Of the 32,000 people who received the Moderna or Pfizer vaccine in a research trial, only one contracted a severe Covid case.
- To what degree do people who never develop symptoms contribute to transmission? Research early in the pandemic suggested that the rate of asymptomatic infections could be as high as 81%. But a meta-analysis, which included 13 studies involving 21,708 people, calculated the rate of asymptomatic presentation to be 17%.
- The accuracy of rapid testing is questioned – and the more accurate test results are not being given in a timely manner.
- Can children widely spread coronavirus? [current thinking is that they are a minor source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- Air conditioning contributes to the pandemic spread.
- It appears that there is increased risk of infection and mortality for those living in larger occupancy households.
- Male patients have almost three times the odds of requiring intensive treatment unit (ITU) admission compared to females.
- Outdoor activities seem to be a lower risk than indoor activities.
- Will other medical treatments for Covid-19 ease symptoms and reduce deaths? So far only remdesivir, Bamlanivimab,
and Regeneron) are approved for treatment. What drugs work?
Arthritis drugs tocilizumab and sarilumab could cut relative risk of death of those in intensive care by 24%
- A current scientific understanding of the way the coronavirus works can be found [here].
There is now a vaccine available – the questions remain:
- how effective it will be in the general population,
- will there be any permanent side effects that will appear months from now,
- how long immunity will last [we can currently say we do not know if it will last more than 4 months],
- there is no evidence the vaccine will block transmission
Heavy breakouts of coronavirus have hit farmworkers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>




