Written by Steven Hansen
The U.S. new cases 7-day rolling average is 8.2 % HIGHER than the 7-day rolling average one week ago. U.S. hospitalizations due to COVID-19 are now 4.4 % HIGHER than the rolling average one week ago. U.S. deaths due to coronavirus are now 16.0 % HIGHER than the rolling average one week ago. Today’s posts include:
- U.S. Coronavirus New Cases are an elevated 210,479
- U.S. Coronavirus hospitalizations are at an elevated 125,544 (for the next 7 days this is the number to watch as new cases and deaths will not be accurately reported)
- U.S. Coronavirus deaths are at 1,394
- U.S. Coronavirus immunizations have been administered to 1.3% of the population
- The 7-day rolling average rate of growth of the pandemic shows new cases worsened, hospitalizations worsened, and deaths worsened
- U.S. could ramp up slow Covid vaccine rollout by giving two half volume doses of Moderna shot
- Nigerian scientist studies country’s coronavirus variant
- CDC Updates Contraindications to COVID-19 Vaccination
- Only 4 states have administered at least half of their Covid-19 doses
- BioNTech Founders Warn of Vaccine Supply Gaps
- Coughing, sneezing, vomiting: Visibly ill people aren’t being kept off planes
- Phone Cameras May Replace Lab Equipment in COVID-19 Testing
- Thinning, Leaky Brain Blood Vessels Seen in COVID-19
- Top US Official Says ‘Growing Body Of Evidence’ Shows COVID-19 Leaked From Chinese Lab
​
The recent worsening of the trendlines for new cases should be attributed to going back to college/university, cooler weather causing more indoor activities, possible mutation of the virus, fatigue from wearing masks / social distancing, holiday activities, political rallies / voting, and continued loosening of regulations designed to slow the coronavirus spread.
My continuing advice is to continue to wash your hands (especially after using the toilet as COVID first sheds in your stool), putting down the toilet seat (as flushing the toilet releases a plume), wear masks, avoid crowds, and maintain social distancing. No handwashing, mask, or social distancing will guarantee you do not get infected – but it sure as hell lowers the risk in all situations – and the evidence to-date shows a lower severity of COVID-19. In addition, certain activities are believed to carry higher risk – like being inside in air conditioning and removing your mask (such as restaurants, around your children/grandchildren, bars, and gyms). It is all about viral load – and outdoor activities are generally safe if you can maintain social distance. Finally, studies show eating right (making sure you are supporting your immune system) and adequate sleep increase your ability to fight off COVID.
include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus1.htm’); ?>
Hospitalizations (grey line) and Mortality (green line)
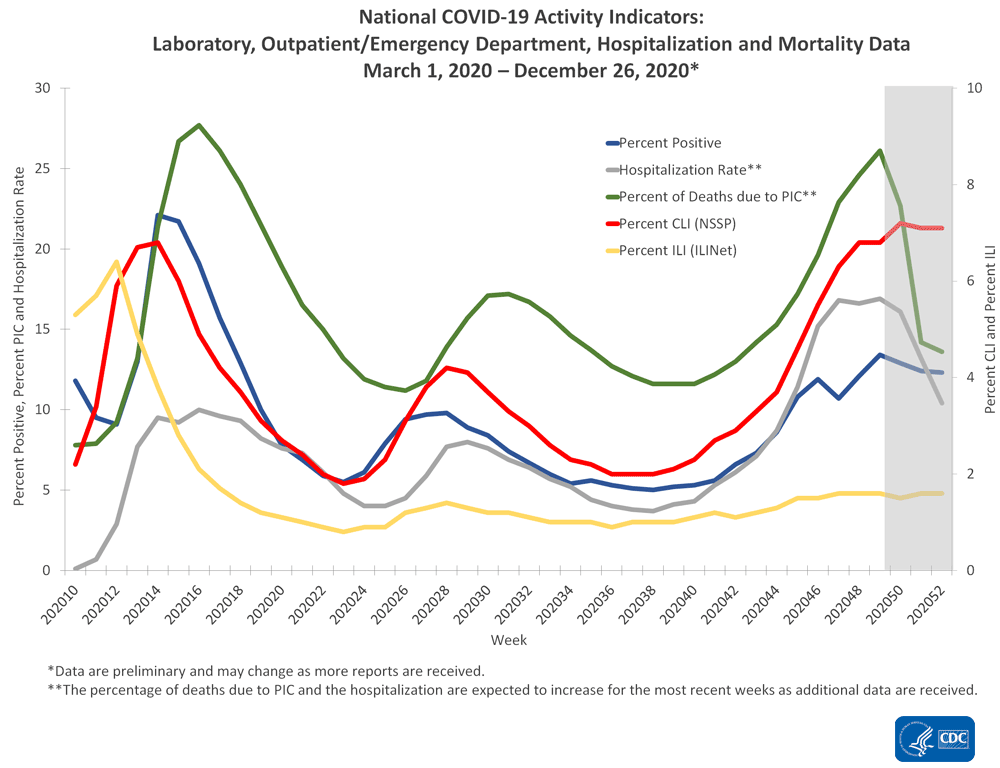
source: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html
The Impact of Holidays – Hospitalizations Are The Only Accurate Gauge As Reporting Is Sporadic
The 4 day Thanksgiving holiday period put a wobble in the trends. Over weekends and holidays, the number of new cases and deaths decline. Over weekends, this is not a problem for week-over-week rolling averages as weekends are compared against the previous weekend. But when a holiday falls within a working week, a non-working day is compared to a working day which causes havok in the trends. Now we are faced with the end of the year holiday season which means reporting is sporadic and numbers will initially look good – and then as the holidays end and the reporting catches up, the numbers will look terrible. In addition, family gatherings and travel will cause more virus transmission.
However, hospitalizations historically appear to be little affected by weekends or holidays – the daily counts do not vary significantly from day-to-day.
The hospitalization growth rate trend is growing at an ever slowing growth rate which is all good news as it means the number of beds needed is currently growing around 4 % every week.

The above graph demonstrates in the last week hospitalization rate of growth has been relatively steady. We have seen that the size of the impact of commingling and travel over the Thanksgiving holiday period – roughly, it seems to have added around 5 % to the rate of growth of new cases, hospitalizations, and deaths.
Historically, hospitalization growth follows new case growth by one to two weeks.
As an analyst, I use the rate of growth to determine the trend. But, the size of the pandemic is growing in terms of real numbers – and if the rate of growth does not become negative – the pandemic will overwhelm all resources.
The graph below shows the rate of growth relative to the growth a week earlier updated through today [note that negative numbers mean the rolling averages are LOWER than the rolling averages one week ago]. As one can see, the rate of growth for new cases peaked in early December 2020 ago and the rate of growth has been decelerating since.

This graph is currently demonstrating that the actions to contain the pandemic are slightly working – but the rate of growth improvement is too slow as we are still seeing some record numbers. In the scheme of things, new cases decline first, followed by hospitalizations, and then deaths.
It is up to each of our readers to protect themselves and others by washing your hands, wearing a mask, avoiding crowds, and maintaining social distancing.
We Are Likely In A Pandemic Surge Caused By The Holidays And Virus Mutation
The “experts” will tell you they told you so – and you should have stayed at home instead of traveling to be with the people you care about. And there is some truth in this opinion.
But there will be no way to accurately understand the impact of the holidays because there are new mutant strains of the coronavirus that are more transmissible.
To gauge the impact of anything, you change ONLY ONE variable at a time (and hopefully in a controlled environment). There are now two variables in play – and it is nearly impossible to separate the impact of each.
Coronavirus News You May Have Missed
Thinning, Leaky Brain Blood Vessels Seen in COVID-19 – MedPage
Microvascular brain injury was seen in COVID-19 patients who died, but no evidence of a direct viral attack on the brain was detected, a pathology report showed.
Damage caused by thinning and leaky brain blood vessels consistently appeared on high-resolution MRI, but there were no signs of SARS-CoV-2 infection in tissue samples, reported Avindra Nath, MD, clinical director of the National Institute of Neurological Disorders and Stroke (NINDS), and co-authors in a New England Journal of Medicine letter.
“We found there were many foci of small blood vessel damage from which there was leakage of blood products into the brain tissue,” Nath said. “The cause of this was not clear but is most likely due to damage from the immune cells or lymphocytes. We found some lymphocytes attached to the endothelial cells in the blood vessels and in the perivascular regions,” he told MedPage Today.
“The inflammatory response is key to the neuropathogenesis of this syndrome, since we were unable to find virus in the brain,” Nath added. “The study potentially has important implications for long-term damage to several structures in the brain, particularly the olfactory bulb and the brainstem.”
Other researchers have found SARS-CoV-2 RNA and protein in the brain and nasopharynx of patients who died with COVID-19, with highest levels of viral RNA found in the olfactory mucous membrane.
Nigerian scientist studies country’s coronavirus variant – AP
A Nigerian scientist has spent the holiday season in his laboratory doing genetic sequencing to learn more about the country’s COVID-19 variant, as cases increase in the country.
Virologist Sunday Omilabu says the information he gathers about the variant will help battle the spread of the disease in Nigeria, Africa’s most populous country with 196 million people.
Nigeria has confirmed 89,163 COVID-19 cases, including 1,302 deaths, according to the figures Sunday from the Africa Centers for Disease Control and Prevention.
“The variants discovered in the U.K. and South Africa, they are distantly different from the variants discovered in Nigeria,” said Omilabu, who said it is not unusual for viruses to mutate and cause variants.
Top US Official Says ‘Growing Body Of Evidence’ Shows COVID-19 Leaked From Chinese Lab – ZeroHedge
The most ‘credible’ theory about the origin of COVID-19 is that it escaped from a Chinese laboratory, according to US National Security Adviser Matthew Pottinger, who made the comment during a Zoom meeting with UK officials.
“There is a growing body of evidence that the lab is likely the most credible source of the virus,” said Pottinger, referring to the Wuhan Institute of Virology, according to the Daily Mail, which notes that ‘even China’s leaders openly admit their previous claims that the virus originated in a Wuhan market are false.’
Pottinger was one of the first US officials to sound the alarm at the White House over the origins of the virus in January 2020, when he initially suspected that the outbreak originated in a Chinese lab – after which Pottinger ordered US intelligence agencies to search for evidence. Good thing he kept this theory to himself, or Twitter may have banned him.
He also slammed the World Health Organization’s probe as a ruse – saying “MPs around the world have a moral role to play in exposing the WHO investigation as a Potemkin exercise,” referring to the facade villages created in 18th Century Crimea to convince the visiting Russian Empress Catherine the Great that the region was doing well.
Iain Duncan Smith, the former Tory Party leader who attended the meeting, said Mr Pottinger’s comments represented a ‘stiffening’ of the US position on the theory that the virus came from a leak at the laboratory, amid reports that the Americans are talking to a whistleblower from the Wuhan institute.
‘I was told the US have an ex-scientist from the laboratory in America at the moment,’ he said. ‘That was what I heard a few weeks ago.
‘I was led to believe this is how they have been able to stiffen up their position on how this outbreak originated.’
He added that Beijing’s refusal to allow journalists to visit the laboratory only served to increase suspicion that it was ‘ground zero’ for the pandemic. ‘The truth is there are people who have been in those labs who maintain that this is the case,’ he said.
‘We don’t know what they have been doing in that laboratory. They may well have been fiddling with bat coronaviruses and looking at them and they made a mistake. I’ve spoken to various people who believe that to be the case.’ –Daily Mail
“Even establishment figures in Beijing have openly dismissed the wet market story,” Pottinger told the call participants.
[editor’s note: if you are interested in this, there are many more juicy tidbits in this post]
The head of the federal government’s Covid-19 vaccine program said Sunday that health officials are exploring the idea of giving a major group of Americans half volume doses of one vaccine to accelerate the rollout.
Moncef Slaoui, the head of Operation Warp Speed, said on CBS’ “Face the Nation” that one way to speed up immunizations against Covid-19 was to give two half-volume doses of the Moderna vaccine to some individuals.
“We know that for the Moderna vaccine giving half the dose for people between the ages of 18 to 55 – two doses, half the dose, which means exactly achieving the objective of immunizing double the number of people with the doses we have – we know it induces identical immune response to the 100 microgram dose,” Slaoui said.
“And therefore, we are in discussions with Moderna and with the FDA – of course ultimately it will be an FDA decision – to accelerate injecting half the volume,” he added.
[editor’s note: also read Trump officials debating cutting Moderna dose in half to speed up COVID-19 vaccination]
Coughing, sneezing, vomiting: Visibly ill people aren’t being kept off planes – Los Angeles Times
Before boarding a flight from Orlando to Los Angeles, Isaias Hernandez filled out a health checklist provided by United Airlines, asserting that he had not been diagnosed with COVID-19 and had not shown any of the disease’s symptoms in the previous two weeks.
But during the flight, the 69-year-old Angeleno collapsed. Three passengers gave him CPR for nearly an hour in the aisle of the plane, and the flight was diverted to Louisiana, where Hernandez was pronounced dead. The coroner’s report listed the cause as “acute respiratory failure, COVID-19.”
The Dec. 14 incident illustrates the deficiencies in the systems that are meant to prevent people from bringing the coronavirus aboard commercial flights and potentially spreading it to the people packed in around them. And it happened as holiday air travel ramped up. In the days surrounding Christmas, more than a million passengers boarded planes almost daily, reaching 1.3 million last Sunday – the most since March.
U.S. airlines boast layers of protocols intended to protect passengers from the virus, including the increased cleaning of plane cabins and a requirement that passengers wear face coverings except when eating or drinking. Nearly all of them also require passengers to fill out a health declaration before boarding. But the only repercussion for lying on the declaration or refusing to wear a mask on the plane is getting banned from the airline, if caught.
… Some U.S. airports, including Los Angeles International Airport, take the extra step of using thermal cameras to gauge people’s temperatures as they enter the terminal, but fliers are allowed to opt out.
The CDC launched an enhanced screening program last January for international passengers arriving to the U.S. from certain countries with widespread transmission of the virus. But it ended the program in November, concluding that the effort failed, partly because COVID-19 has too many symptoms that are also common to other illnesses; travelers could mask their symptoms to avoid detection; and even travelers with no symptoms can still carry and spread the virus.
What is needed, passenger rights advocates, flight attendant unions and academics say, is for the U.S. Department of Transportation to adopt uniform standards for airline safety, including a mask mandate that is enforced with steep fines. They also call on the federal agency to put more resources into contact tracing of known cases and improved access to quick and reliable COVID-19 tests that passengers can take before a flight.
CDC Updates Contraindications to COVID-19 Vaccination – MedPage
Anyone with a history of immediate allergic reaction of any severity to any component of mRNA COVID-19 vaccines or to polysorbate should not be vaccinated, the CDC said in updated interim guidance.
While previously the agency released guidelines for contraindication to vaccination, it’s now broadened to include those with a history of immediate allergic reaction to a previous dose of or any component of mRNA COVID-19 vaccines, including polyethylene glycol.
In addition, people developing severe allergic reactions such as anaphylaxis after a first dose of mRNA COVID-19 vaccine should not receive a second dose.
All ingredients in the Pfizer/BioNTech and Moderna vaccines were listed by CDC in an “interim clinical considerations” document posted on the agency’s website (see Appendix B). Polysorbate is not a vaccine ingredient but was included because people sensitive to it may also react to polyethylene glycol.
People with allergy histories involving these substances should be considered for allergist/immunologist referral to determine if they can receive the vaccine, the agency said in a call with clinicians.
“This guidance is being updated primarily because starting in a few days, people who got their first dose will be eligible to receive a second dose and we thought providers needed more guidance,” said the CDC’s Sarah Mbaeyi, MD, on the call. “We are continuously reevaluating our guidelines to make sure they are based on the best available information, so providers had more information available when people started coming in for their second dose of vaccines.”
[editor’s note: the following is Appendix B:]
Ingredients included in Pfizer-BioNTech and Moderna mRNA COVID-19 vaccines
Description Pfizer-BioNTech COVID-19 vaccine Moderna COVID-19 vaccine mRNA Nucleoside-modified mRNA encoding the viral spike (S) glycoprotein of SARS-CoV-2 Nucleoside-modified mRNA encoding the viral spike (S) glycoprotein of SARS-CoV-2 Lipids 2[(polyethylene glycol)-2000]-N,N-ditetradecylacetamide PEG2000-DMG: 1,2-dimyristoyl-rac-glycerol, methoxypolyethylene glycol 1,2-distearoyl-sn-glycero-3-phosphocholine 1,2-distearoyl-sn-glycero-3-phosphocholine Cholesterol Cholesterol (4-hydroxybutyl)azanediyl)bis(hexane-6,1-diyl)bis(2-hexyldecanoate) SM-102: heptadecan-9-yl 8-((2-hydroxyethyl) (6-oxo-6-(undecyloxy) hexyl) amino) octanoate Salts, sugars, buffers Potassium chloride Tromethamine Monobasic potassium phosphate Tromethamine hydrochloride Sodium chloride Acetic acid Dibasic sodium phosphate dihydrate Sodium acetate Sucrose Sucrose * Neither vaccine contain eggs, gelatin, latex, or preservatives
Note: Both the Pfizer-BioNTech and Moderna COVID-19 vaccines contain polyethylene glycol (PEG). PEG is a primary ingredient in osmotic laxatives and oral bowel preparations for colonoscopy procedures, an inactive ingredient or excipient in many medications, and is used in a process called pegylation to improve the therapeutic activity of some medications (including certain chemotherapeutics). Additionally, cross-reactive hypersensitivity between PEG and polysorbates (included as an excipient in some vaccines and other therapeutic agents) can occur.
BioNTech Founders Warn of Vaccine Supply Gaps – Medscape
BioNTech is working flat out with partner Pfizer to boost production of their COVID-19 vaccine, its founders said, warning there would be gaps in supply until other vaccines were rolled out.
The German biotech startup has led the vaccine race but its shot has been slow to arrive in the European Union because of relatively late approval from the bloc’s health regulator and the small size of the order placed by Brussels.
The delays in rolling out the home-grown vaccine have caused consternation in Germany, where some regions had to halt vaccinations within days of starting an inoculation drive.
“At the moment it doesn’t look good – a hole is appearing because there’s a lack of other approved vaccines and we have to fill the gap with our own vaccine,” BioNTech CEO Ugur Sahin told news weekly Spiegel.
Sahin founded BioNTech with his wife, Oezlem Tuereci, who is the company’s chief medical officer. Both faulted the EU’s decision to spread orders in the expectation that more vaccines would be approved quickly.
The United States ordered 600 million doses of the BioNTech/Pfizer shot in July, while the EU waited until November to place an order half that size.
“At some point it became clear that it would not be possible to deliver so quickly,” Tuereci told Spiegel. “By then it was already too late to place follow-on orders.”
Phone Cameras May Replace Lab Equipment in COVID-19 Testing – Reuters
Researchers seeking faster, more convenient options for ramping up coronavirus testing are looking at a novel approach using a gene-editing technology called CRISPR and smartphone cameras in place of bulky laboratory equipment.
In a paper published in Cell, a team that includes Jennifer Doudna – this year’s co-winner of the Nobel Prize in chemistry – describes a CRISPR-based COVID-19 test in which the swab sample is mixed with an enzyme called Cas13 that can recognize the genetic material of the new coronavirus, plus an extra molecule that becomes fluorescent when cut.
The mixture is then placed in a device that attaches to smartphones. If the mixture contains genetic material from the virus, the enzyme finds it and slices it – without time-consuming virus-purification steps other tests require. The enzyme also slices the extra molecule, and the resulting fluorescence is detected by the phone camera as a signal that the virus is present.
Smartphone cameras “are about 10-fold more sensitive than lab-based devices in detecting the fluorescence signal fast and reliably within minutes,” said coauthor Dr. Melanie Ott of the Gladstone Institute of Virology at the University of California, San Francisco. “The cell phone is also portable, widely available and… via GPS can facilitate contact tracing.”
Unclear If COVID Vaccine Will Work on South African Strain: Top Scientist Sir John Bell – Newsweek
A top vaccine scientist has said it is still unclear whether current vaccines will be effective against a new variant of the novel coronavirus that was first detected in South Africa.
John Bell, a professor who led the development of the AstraZeneca-University of Oxford COVID-19 vaccine, told Times Radio that the South African variant-dubbed 501.V2-worried him more than another strain recently detected in the United Kingdom “by some margin.”
Like the U.K. variant, the South African strain also appears to be more transmissible than the original. First detected in December, it has now been identified in a handful of other countries around the world, including France and Japan.
Both of the new variants, which share some similarities, have multiple genetic mutations, but the South African one features significant changes to the important “spike” protein that enables the SARS-CoV-2 virus to infect human cells.
These changes could potentially make vaccines less effective against this variant, according to Bell, although more research needs to be conducted in order to properly understand this issue.
… Bell said that scientists were now looking at the “crucial question” of whether or not vaccines will be effective against the new variants detected in the U.K. and South Africa-neither of which appear to cause more serious disease.
“I can’t give you an insight now,” Bell said. “My gut feeling is that I think the vaccine will be still effective against the [U.K.] strain. And I don’t know about the South African strain. I think that’s a there’s a big question mark about that.”
Bell said there is still some headroom with the vaccines that are currently available, because they work “much better” than anyone would have predicted previously.
“We do have some room to manoeuvre if they worked 20 percent less well because of mutation. We’d still have good vaccines in my view. I think it’s unlikely that these mutations will turn off the effect of vaccines entirely, I think you’ll still have a residual effect,” Bell said.
If necessary, Bell said that it was “perfectly possible” to tweak existing vaccines so that they are effective against the new strain and that this would not take a whole year.
[editor’s note: also read Covid variant in South Africa is ‘more of a problem’ than the one in UK, official says]
British Prime Minister Boris Johnson said England is adopting a national lockdown that he hopes will be tough enough to contain a new, highly contagious variant of Covid-19.
In an announcement Monday evening, Johnson said primary, secondary and colleges will also move to remote learning in most cases.
[editor’s note: this appears to be a Tier 5 national lockdown which is the same as the one last March and will be in effect until at least mid-February. All nonessential shops and personal care services like hairdressers will be closed, and restaurants can only operate takeout services.]
A neutralizing antibody treatment for COVID-19 – bamlanivimab – injection 700 mg/20 mL – Lilly
[editor’s note – a nurse friend reminded me about “BAM”, suggesting it was an effective option to avoid hospitalization.]
If you’ve recently been diagnosed with COVID-19, you may have a new treatment option: bamlanivimab (bam-la-NIV-i-mab). The research so far shows that for certain people, taking this drug may help limit the amount of virus in the body. This may help their symptoms improve sooner – and they may be less likely to need to go to the hospital. But bamlanivimab is a new drug that’s still being studied, so there’s a lot that scientists don’t know about the benefits and risks.
Here, you’ll learn about COVID-19 and this new treatment – including its possible benefits and side effects. Together, you and your doctor can decide if this treatment is right for you.
Bamlanivimab is an investigational medicine used for the treatment of COVID-19 in non-hospitalized adults and adolescents 12 years of age or older with mild to moderate symptoms who weigh 88 pounds (40 kg) or more, and who are at high risk for developing severe COVID-19 symptoms or the need for hospitalization.
- Bamlanivimab has not been approved, but has been authorized for emergency use by FDA
- Bamlanivimab is authorized only for the duration of the declaration that circumstances exist justifying the authorization of the emergency use of the bamlanivimab under Section 564(b)(1) of the Act, 21 U.S.C. 360bbb-3(b)(1), unless the authorization is terminated or revoked sooner.
For information on the authorized use of bamlanivimab and mandatory requirements under the Emergency Use Authorization, please review the Fact Sheet for Patients, Parents and Caregivers (English) or Fact Sheet for Patients, Parents and Caregivers (Spanish).
Only 4 states have administered at least half of their Covid-19 doses, CDC data shows – CNN
Fewer than 30% of the 15.4 million Covid-19 vaccine doses distributed in the US have been administered, according to data from the Centers for Disease Control and Prevention.
The figures, last updated Monday, show a slight slowdown in the rate of vaccine administration. As of Saturday morning, the rate was closer to 33% administered.
Only four states have administered at least half of the Covid-19 vaccine doses that have been distributed to them, according to the CDC data. Those states are: South Dakota, North Dakota, Tennessee and Connecticut.
Meanwhile, in 12 states, fewer than a quarter of the doses distributed have been administered.
- Kansas: 15.3%
- Georgia: 15.5%
- Arizona: 16.1%
- Louisiana: 22.7%
- Virginia: 23.2%
- Florida: 23.3%
- Washington: 23.8%
- Maryland: 23.9%
- Oregon: 24.1%
- California: 24.2%
- Nevada: 24.3%
- Alabama: 24.8%
The following are foreign headlines with hyperlinks to the posts
Britain has taken another giant step in the fight against COVID-19, ramping up its immunization program by giving out the first shots in the world from the vaccine created by Oxford University and pharmaceutical giant AstraZeneca.
The U.K.’s independent Scientific Advisory Group for Emergencies (SAGE) has conditionally backed the U.K.’s decision to delay administering a second dose of the coronavirus vaccine developed by Pfizer and BioNTech.
Britain begins giving clinically authorized and tested Oxford-AstraZeneca shots.
India will not allow the export of the Oxford University-AstraZeneca vaccine for several months, the head of Serum Institute of India, which has been contracted to make 1 billion doses of the vaccine for developing nation
Beijing Reports Tens Of Thousands Inoculated In 1st Days Of COVID-19 Vaccine Campaign
Nigeria is seeing more infections of COVID-19 but it is not yet certain if that is from the variant, said Omilambu, the director of the Center for Human and Zoonotic Virology at the Lagos University College of Medicine and Teaching Hospital.
“What we could say clinically is that we have more people coming down with severe signs and symptoms,” he said, describing how one person can spread the disease to four or five family members, which is a higher rate of transmission than had been recorded earlier.
Scotland entering new lockdown until end of January
North Korea asks for COVID-19 vaccines from international alliance: report
North Korean state newspaper calls for tightening of Covid measures ahead of party congress
India defends the decision to approve a homegrown vaccine before trials finish.
A Swedish official advised people to stay home for Christmas, then flew to Spain.
Japan is considering declaring a state of emergency for the Greater Tokyo metropolitan area as the number of Covid-19 cases surge, Reuters reports. The move would cast fresh doubt over whether the country can push ahead with the Olympics this year while keeping economic damage to a minimum, according to Reuters. Kyodo News, citing sources, reported that the state of emergency would take effect on Jan. 9 and last about a month.
Japan’s PM says Covid-19 vaccinations will begin in late February
New UK variant detected in at least 37 countries
German police struggle to keep skiers away despite nationwide lockdown
Thailand reports largest daily increase in new Covid-19 cases since start of pandemic
The following additional national and state headlines with hyperlinks to the posts
More than 1.3 million travelers passed through U.S. airports Sunday, a new pandemic travel record as passengers headed from the holidays.
TSA screens more than 3 million travelers over New Year’s weekend
An outbreak at a convent near Albany, N.Y., has infected nearly half of its roughly 100 residents. Nine sisters, all older than 80, died of Covid-19 in December.
An inflatable holiday-themed costume may be behind an outbreak at a California hospital. An employee wore an “air-powered” costume on Christmas Day, and within days 44 staffers had tested positive.
Colleges offer ‘mini-mester’ and career boot camps over winter breaks extended because of COVID-19
NCAA Says 2021 Men’s March Madness Will Take Place In A Bubble In Indiana
Symptom Screening, Isolated Spaces Could Reduce COVID-19 at Homeless Shelters
Children May Be Missing Vaccinations During Pandemic
Minority Children More Likely Than Whites to Be Infected With SARS-CoV-2
Fauci Says Life May Be ‘Quite Normal’ by Fall With 1M Daily COVID Vaccines
Cuomo threatens to fine hospitals if they don’t step up the pace of vaccinations.
New York Gov. Andrew Cuomo said he plans to propose a law that would make it a crime to sell or administer coronavirus vaccine shots to people who are trying to skip ahead in line.
Moderna is upping the minimum number of doses it expects to make this year by 20% to 600 million, the company said in a statement.
BioNTech and Pfizer warned that they had no evidence that their jointly developed vaccine will continue to protect against Covid-19 if the booster shot is given later than the amount of time tested in trials, Reuters reports.
As Covid cases surge in California, Hollywood pauses TV production
130 New York City school buildings are closed due to Covid-19 cases
US CDC hopes to double the number of coronavirus samples checked for new mutations
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
November 2020 Construction Spending Again Improves
Covid19 Europe Update 02 January 2021
3 Fallacies That Blighted This Year’s COVID Commentary – Have You Fallen Foul Of Any Of Them?
How Pandemics Past And Present Fuel The Rise Of Large Companies
Warning to Readers
The amount of politically biased articles on the internet continues to increase. And studies and opinions of the experts continue to contradict other studies and expert opinions. Honestly, it is difficult to believe anything anymore. A study usually cannot establish cause and effect – but only correlation. Be very careful what you believe about this pandemic.

I assemble this coronavirus update daily – sifting through the posts on the internet. I try to avoid politically slanted posts (mostly from CNN, New York Times, and the Washington Post) and can usually find unslanted posts on that subject from other sources on the internet. I wait to publish posts on subjects that I cannot validate across several sources. But after all this extra work, I do not know if I have conveyed the REAL facts. It is my job to provide information so that you have the facts necessary – and then it is up to readers to draw conclusions.
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19 when recovering from COVID-19. Herd immunity does not look like an option without immunization although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a significantly higher death rate as there is relatively few hospitalizations and deaths in younger age groups..
- There are at least 8 strains of the coronavirus. New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
What we do or do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work.
- Do we develop lasting immunity to the coronavirus? Another coronavirus – the simple cold – does not develop long term immunity. However, How Many Americans Are Immune From COVID? Research into the coronavirus is running way behind the need for answers. Whilst we strive for herd immunity through vaccination – we lack an understanding of the general immunity people might have to the pandemic. This will affect the point herd immunity can be reached. The following articles discuss immunity: Can the Common Cold Help Protect You from COVID-19?, Does the Common Cold Protect You from COVID-19?, Immune cells for the common cold may recognize SARS-CoV-2
- To what degree do people who never develop symptoms contribute to transmission? Research early in the pandemic suggested that the rate of asymptomatic infections could be as high as 81%. But a meta-analysis, which included 13 studies involving 21,708 people, calculated the rate of asymptomatic presentation to be 17%.
- The accuracy of rapid testing is questioned – and the more accurate test results are not being given in a timely manner.
- Can children widely spread coronavirus? [current thinking is that they are a minor source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- Air conditioning contributes to the pandemic spread.
- It appears that there is increased risk of infection and mortality for those living in larger occupancy households.
- Male patients have almost three times the odds of requiring intensive treatment unit (ITU) admission compared to females.
- Outdoor activities seem to be a lower risk than indoor activities.
- Will other medical treatments for Covid-19 ease symptoms and reduce deaths? So far only remdesivir, Bamlanivimab,
and Regeneron) are approved for treatment. What drugs work?
- A current scientific understanding of the way the coronavirus works can be found [here].
There is now a vaccine available – the questions remain:
- how effective it will be in the general population,
- will there be any permanent side effects that will appear months from now,
- how long immunity will last [we can currently say we do not know if it will last more than 4 months],
- there is no evidence the vaccine will block transmission
Heavy breakouts of coronavirus have hit farmworkers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>





