
Written by Steven Hansen
The U.S. new cases 7-day rolling average are 5.2 % LOWER than the 7-day rolling average one week ago. U.S. hospitalizations due to COVID-19 are now 4.0 % HIGHER than the rolling average one week ago. U.S. deaths due to coronavirus are now 1.4 % LOWER than the rolling average one week ago. Today’s posts include:
- U.S. Coronavirus New Cases are at an elevated 192,081
- U.S. Coronavirus hospitalizations are at a record 120,151
- U.S. Coronavirus deaths are at an elevated 2,899
- U.S. Coronavirus immunizations are 9,465,725 doses distributed and 1,008,025 doses administered as of 23 December
- The 7-day rolling average rate of growth of the pandemic shows new cases improved, hospitalizations improved, and deaths improved
- Iran gets clearance to buy vaccine, despite sanctions.
- Fauci Says U.S. Herd Immunity Is Reachable if Up to 90% Receive Vaccine
- U.S. Now Requires All U.K. Travelers To Have A Negative Coronavirus Test
- Tennessee Emerges as New COVID-19 Epicenter in US
- Southern states are overwhelmed by virus cases after dodging the fall surge
- More Than Half of Americans Would Support National One-Month Lockdown
- Testing delays, staff shortages impede distribution of Covid treatment used by Trump
- Are two phases of quarantine better than one?
- Marsh & McLennan CEO expects mandatory Covid vaccinations to be very rare

The recent worsening of the trendlines for new cases should be attributed to going back to college/university, cooler weather causing more indoor activities, possible mutation of the virus, fatigue from wearing masks / social distancing, holiday activities, political rallies / voting, and continued loosening of regulations designed to slow the coronavirus spread.
My continuing advice is to continue to wash your hands (especially after using the toilet as COVID first sheds in your stool), putting down the toilet seat (as flushing the toilet releases a plume), wear masks, avoid crowds, and maintain social distancing. No handwashing, mask, or social distancing will guarantee you do not get infected – but it sure as hell lowers the risk in all situations – and the evidence to-date shows a lower severity of COVID-19. In addition, certain activities are believed to carry higher risk – like being inside in air conditioning and removing your mask (such as restaurants, around your children/grandchildren, bars, and gyms). It is all about viral load – and outdoor activities are generally safe if you can maintain social distance. Finally, studies show eating right (making sure you are supporting your immune system) and adequate sleep increase your ability to fight off COVID.
include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus1.htm’); ?>
Hospitalizations (grey line) and Mortality (green line)
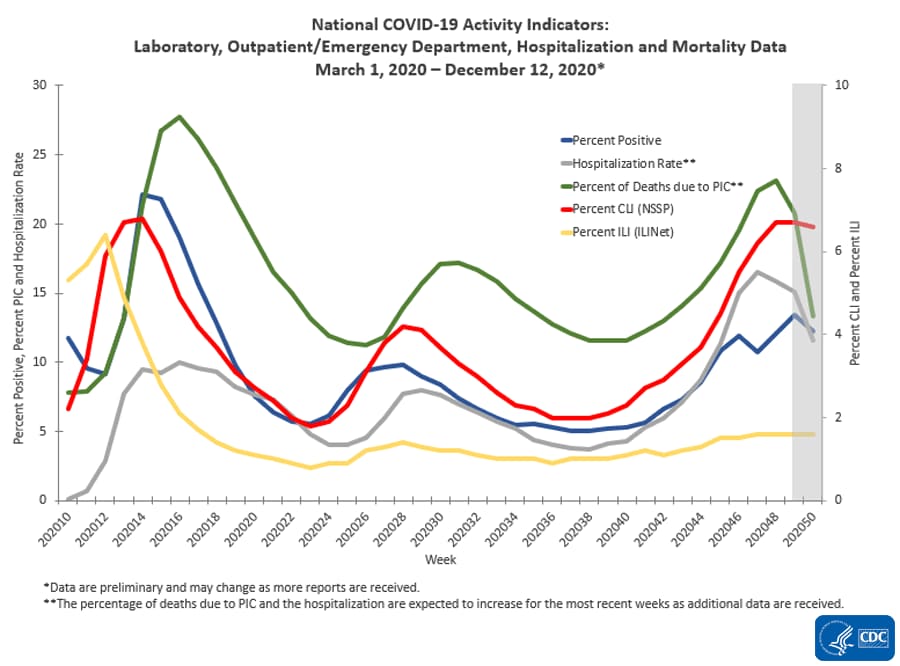
source: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html
The Impact of Holidays
The 4 day Thanksgiving holiday period put a wobble in the trends. Over weekends and holidays, the number of new cases and deaths decline. Over weekends, this is not a problem for week-over-week rolling averages as weekends are compared against the previous weekend. But when a holiday falls within a working week, a non-working day is compared to a working day which causes havok in the trends. Now we are faced with the end of year holiday season which means reporting is sporadic and numbers will initially look good – and then as the holidays end and the reporting catches up, the numbers will look terrible. In addition, family gatherings and travel will cause more virus transmission.
However, hospitalizations historically appear to be little affected by weekends or holidays – the daily counts do not vary significantly from day-to-day.
The hospitalization growth rate trend is growing at an ever slowing growth rate which is all good news as it means the number of beds needed is currently growing around 4 % every week.

The above graph demonstrates in the last week hospitalization rate of growth has been relatively steady. We have seen that the size of the impact of commingling and travel over the Thanksgiving holiday period – roughly, it seems to have added around 5 % to the rate of growth of new cases, hospitalizations, and deaths.
Historically, hospitalization growth follows new case growth by one to two weeks.
As an analyst, I use the rate of growth to determine the trend. But, the size of the pandemic is growing in terms of real numbers – and if the rate of growth does not become negative – the pandemic will overwhelm all resources.
The graph below shows the rate of growth relative to the growth a week earlier updated through today [note that negative numbers mean the rolling averages are LOWER than the rolling averages one week ago]. As one can see, the rate of growth for new cases peaked over one month ago and the rate of growth has been decelerating.

This graph is currently demonstrating that the actions to contain the pandemic are slightly working – but the rate of growth improvement is too slow as we are still seeing some record numbers. In the scheme of things, new cases decline first, followed by hospitalizations, and then deaths.
It is up to each of our readers to protect themselves and others by washing your hands, wearing a mask, avoiding crowds, and maintaining social distancing.
Coronavirus News You May Have Missed
Testing delays, staff shortages impede distribution of Covid treatment used by Trump – CNBC
- Monoclonal antibody treatments have shown promising signs in fighting the disease if given early on in infection.
- But the drugs aren’t being widely used by the general public.
- A shortage of staff that can administer the drugs, which have to be given via IV drips, combined with delays in Covid-19 testing have limited their use.
U.S. Now Requires All U.K. Travelers To Have A Negative Coronavirus Test – NPR
The Centers for Disease Control and Prevention announced Thursday that all travelers coming from the United Kingdom must present a negative coronavirus test no more than 72 hours before taking a flight to the U.S.
The new mandate comes after a new variant of the coronavirus spread across England. So far, the new variant, which contains 17 mutations, appears more transmissible and harder to control. England reported a new record of confirmed COVID-19 cases, now reaching more than 2.1 million cases on Thursday, according to Johns Hopkins University.
This move by the CDC falls short of an all-out ban to U.K. travelers that other countries, including Canada and many European nations, have implemented following news of the variant’s outbreak.
This decision follows an executive order signed by President Trump on March 14 that suspended the entry of foreign nationals who visited the U.K. in the previous 14 days. That reduced air travel between the two countries to about 90%.
“This additional testing requirement will fortify our protection of the American public to improve their health and safety and ensure responsible international travel,” the CDC said in a statement.
Under these new rules, passengers must get a viral test that can detect current infections within three days of their flight. Travelers must then provide airlines with documentation of their results. The CDC order is set to be signed Christmas Day, and will become effective Dec. 28.
Tennessee Emerges as New COVID-19 Epicenter in US – Medscape/Reuters
Tennessee emerged on Wednesday as an epicenter of the latest COVID-19 surge as U.S. political leaders sought to guard against a highly contagious variant sweeping across Britain.
The southern state averaged nearly 128 new infections per 100,000 people over the last seven days, the highest state rate in the country, according to U.S. Centers for Disease Control and Prevention data. It was followed by California at 111 new cases per 100,000 residents.
“Our state is ground zero for a surge in COVID-19 and we need Tennesseans to (do) their part,” Tennessee Governor Bill Lee said on Twitter with a graphic stating: “Tennessee cannot sustain another holiday surge.”
Public health officials believe that Americans traveling and gathering for the Thanksgiving holiday contributed to the latest explosion in cases.
All told 31 U.S. states have reported a grim record in new COVID-19 infections for December as hospitalizations and deaths also spiral. More than 194,600 new cases were confirmed on Tuesday alone.
Americans who saw a ray of hope in the release of two vaccines in December learned of an even more transmissible coronavirus variant spreading in the United Kingdom, which has not been fully tested against the inoculations.
Southern states are overwhelmed by virus cases after dodging the fall surge. – New York Times
As many Americans are winding down for the holidays, an explosion of coronavirus cases and deaths across the nation is hitting with perilous force, particularly in the South, which avoided much of the fall surge.
Six Southern states have seen sustained case increases in the last week: Tennessee, Alabama, Georgia, South Carolina, Florida and Texas.
Tennessee reported the country’s most cases per 100,000 people on average over the last seven days, and Alabama set a single-day death record for the state on Wednesday, with 135, according to a New York Times database. In Florida, a virus surge in the past week means cases could soon surpass the state’s summer peak.
These increases are not just indicative of more testing. Florida’s more than 20 percent rise in cases over the last two weeks matches the growth in hospitalizations, although far fewer residents are hospitalized now than in the summer. In Texas, which has also had an upswing of more than 20 percent over the same time period, Dallas County has added more than 15,000 cases in the last week, a record.
Brazil institute says CoronaVac efficacy above 50%, but delays full results – Reuters
Brazilian researchers said on Wednesday the COVID-19 vaccine developed by China’s Sinovac Biotech is more than 50% effective based on trial data, but again withheld full results at the company’s request, raising questions about transparency.
Brazil is the first country to complete a late-stage trial of the vaccine, called CoronaVac, but a release of the results, first set for early December, has now been delayed three times.
The latest delay is a blow to Beijing, which has been racing to catch up with Western drugmakers, and will add to criticism that Chinese vaccine makers have lacked transparency.
It is also likely to fan growing skepticism toward the Chinese vaccine in Brazil, just as the virus roars back to life. President Jair Bolsonaro, a coronavirus skeptic who has said he will not take a COVID-19 vaccine, has repeatedly questioned the Chinese vaccine based on its “origins.” A poll earlier this month showed that half of Brazilians now reject it.
Officials from the Sao Paulo state government’s Butantan Institute declined to specify the efficacy rate from a trial they led with 13,000 volunteers, citing contractual obligations with Sinovac. They said, however, the vaccine was effective enough against the novel coronavirus for it to be approved for emergency use in Brazil. Health regulator Anvisa has stipulated an efficacy rate of at least 50% for vaccines in the pandemic.
[editor’s note: the following post tells a different story of the effective rate of the Sinovac vaccine]
Turkey says China’s Sinovac COVID vaccine 91.25% effective in late trials – Reuters
A COVID-19 vaccine developed by China’s Sinovac Biotech is 91.25% effective, according to interim data from a late-stage trial in Turkey, a potentially much better result than reported from a separate trial of the vaccine in Brazil.
Researchers in Brazil, which is also running a final Phase III trial of the vaccine, said on Wednesday the shot was more than 50% effective, but withheld full results at the company’s request, raising questions about transparency.
Turkish researchers said on Thursday no major side-effects were seen during their trial, apart from one person who had an allergic reaction. Common adverse effects caused by the vaccine were fever, mild pain and slight fatigue, they said.
The Turkish trials began on Sept. 14 and have included more than 7,000 volunteers, the researchers said, adding the results announced on Thursday were based on data from 1,322 people.
Sinovac is the first Chinese vaccine maker to release details from late-stage clinical trials, following positive results from rival products developed by Pfizer, Moderna and AstraZeneca last month.
The Turkish researchers, speaking alongside Health Minister Fahrettin Koca, said 26 of the 29 people who were infected during the trial were given placebos, adding the trial would continue until 40 people become infected.
“We are now certain that the vaccine is effective and safe (to use) on Turkish people,” Koca said, adding Ankara would use the data for licensing the vaccine.
He also said that researchers initially planned to announce the results after 40 people were infected, but that the findings showed the volunteers had minimal adverse effects after the shot and that it was therefore deemed safe.
“Despite it being risky, we saw a very light picture where three people’s PCR (COVID test) were positive, with no fever or respiratory problems… We can easily say that despite it being risky, those three people went through it very lightly,” he said.
Turkey had agreed to buy 50 million doses of Sinovac’s shot and receive delivery by Dec. 11 but the shipment was delayed.
Koca said three million doses would arrive on Monday, adding that Turkey would vaccinate some nine million people in the first group, starting with health workers.
Chinese vaccines are poised to fill gap, but will they work? – AP
With rich countries snapping up supplies of COVID-19 vaccines, some parts of the world may have to rely on Chinese-developed shots to try to conquer the outbreak. The question: Will they work?
There is no outward reason to believe they won’t, but China has a history of vaccine scandals, and its drugmakers have revealed little about their final human trials and the more than 1 million emergency-use inoculations they say have been carried out inside the country already.
Wealthy nations have reserved about 9 billion of the 12 billion mostly Western-developed shots expected to be produced next year, while COVAX, a global effort to ensure equal access to COVID-19 vaccines, has fallen short of i ts promised capacity of 2 billion doses.
For those countries that have not yet secured a vaccine, China may be the only solution.
China has six candidates in the last stage of trials and is one of the few nations that can manufacture vaccine on a large scale. Government officials have announced a capacity of 1 billion doses next year, with President Xi Jinping vowing China’s vaccines will be a boon to the world.
The potential use of its vaccine by millions of people in other countries gives China an opportunity both to repair the damage to its reputation from an outbreak that escaped its borders and to show the world it can be a major scientific player.
Yet past scandals have damaged its own citizens’ trust in its vaccines, with manufacturing and supply chain problems casting doubt on whether it can really be a savior.
“A question mark remains over how China can ensure the delivery of reliable vaccines,” said Joy Zhang, a professor who studies the ethics of emerging science at the University of Kent in Britain. She cited China’s “non-transparency over scientific data and a troubled history with vaccine delivery.”
Virus ‘Endemic,’ Expect More Variants, Vaccine Tweaks – Medscape
After a new, potentially more easily transmissible genetic variant of SARS-CoV-2 was reported in the United Kingdom, several scientists have said that current vaccines are likely to protect against the new variant, and vaccine manufacturers are running tests to make sure.
But as a larger proportion of the global population becomes immune to SARS-CoV-2 through infection or vaccination, the virus will likely evolve to escape that immunity, and vaccines may need to be updated, Edward Holmes, PhD, told Medscape Medical News.
“I can’t predict what mutations will appear in what order at what time, but I can make a pretty sure prediction it’s going to evolve and escape immunity like everything always does,” said Holmes, an evolutionary virologist at the University of Sydney, Sydney, Australia, who was involved in mapping the SARS-CoV-2 genome. “That’s an inevitable consequence of natural selection. It’s been played out for millennia and will happen again.”
Research will show whether current vaccines are still highly effective against the newly reported variants. If they are, “we can breathe a small sigh of relief,” Holmes told Medscape Editor-in-Chief Eric Topol, MD, leader of the Scripps Translational Science Institute in La Jolla, California, in an upcoming episode of One-on-One Interviews. Other virologists and vaccinologists have tweeted in recent days that they anticipate that the new variant is likely not sufficiently different to make current vaccines ineffective.
… There’s evidence that viral loads are heavier in people infected with the UK variant, as indicated by lower average cycle threshold values for PCR tests and more sequence reads when samples are sequenced, Holmes said. This would explain the new variant’s faster growth.
More Than Half of Americans Would Support National One-Month Lockdown – Newsweek
Most Americans would support a one-month-long lockdown in order to curb the spread of COVID-19, recent poll data indicated.
As the U.S. enters what President-elect Joe Biden has referred to as a “dark winter,” cases of COVID-19 have increased nationwide. In response, some states have enacted business closures and restrictions in the number of individuals that can gather together. Despite the ongoing COVID threat, Biden has said that his coronavirus response plan does not include a nationwide lockdown.
“I’m not going to shut down the economy,” Biden said in November. “I’m going to shut down the virus.”
Despite Biden’s reluctance, some Americans believe that staying at home for one month may not be such a bad idea. According to a poll released by Vox and Data for Progress on Thursday, 52 percent of likely voters said they would support a one-month lockdown.
That poll result jibes with the results of a November YouGov poll in which 64 percent of Americans would support a temporary lockdown in their states. While 87 percent of Democrats polled would be in favor of the lockdown, only 30 percent of Republicans that participated in the poll supported the idea.
Fauci Says U.S. Herd Immunity Is Reachable if Up to 90% Receive Vaccine – Newsweek
Dr. Anthony Fauci, the nation’s leading infectious diseases expert, said that herd immunity in the U.S. could be reached if up to 90 percent of Americans receive a COVID-19 vaccine.
Speaking to The New York Times on Thursday, Fauci, who is the director of the National Institute of Allergy and Infectious Diseases, said, “We really don’t know what the real number is. I think the real range is somewhere between 70 to 90 percent. But I’m not going to say 90 percent.”
He added, “We need to have some humility here.”
Earlier in the pandemic, Fauci suggested that a smaller percentage of Americans would have to receive a vaccine to reach herd immunity, a term used to describe widespread protection from the coronavirus across the country.
As the Times noted, Fauci previously said that “70, 75 percent” of the population would need to be vaccinated for the U.S. to attain herd immunity, but last week he suggested a higher percentage was needed.
“If you really want true herd immunity, where you get a blanket of protection over the country…you want about 75 to 85 percent of the country to get vaccinated,” Fauci told Vox’s Today, Explained podcast on December 15. “I would say even closer to 85 percent.”
He made similar comments a day later, during an interview on CNBC’s Healthy Returns livestream. “I would think that you would need somewhere between 70, 75, maybe 80 percent of the population vaccinated. The number that I’ve been using, again it’s an estimate,” he said.
Asked why he has increased the vaccine percentage needed to reach herd immunity, Fauci told the Times, “When polls said only about half of all Americans would take a vaccine, I was saying herd immunity would take 70 to 75 percent. Then, when newer surveys said 60 percent or more would take it, I thought, I can nudge this up a bit, so I went to 80, 85.”
[editor’s note: I believe Dr. Fauci is the wrong person to listen to as he has continuously migrated positions. It is the blind leading the blind]
Iran gets clearance to buy vaccine, despite sanctions. – New York Times
Iran has received approval from the United States to buy nearly 17 million doses of the coronavirus vaccine, its central bank governor said Thursday, a transaction that Iranian officials said had been previously blocked by American sanctions.
The central bank governor, Abdolnaser Hemmati, said that the country had designated $244 million to purchase the vaccines and that it had received assurances that the U.S. would grant a sanctions exemption for the payment.
But Mr. Hemmati told state television that sanctions remained an obstacle for Iran to purchase medicine and that several attempts at paying through a bank in Switzerland had failed.
The American sanctions, aimed at forcing Iran to rein in its nuclear program and curb its support for militias in the region, exempt humanitarian aid and medicine. But international banks, skittish about running afoul of the sanctions, have generally blocked any transaction involving Iran.
In recent days, a coalition of international rights groups had called on the United States to issue an assurance to banks that they would not face sanctions for transactions involving Iranian vaccine purchases.
Mr. Hemmati said the U.S. had granted the permission “under the pressure of world public opinion.”
Are two phases of quarantine better than one? – EurekAlert
New research into this question shows that the second wave of an epidemic is very different if a population has a homogenous distribution of contacts, compared to the scenario of subpopulations with diverse number of contacts.
The research, by American authors from Oakland University, Novi High School, and California Polytechnic State University, used a simulation approach to model the progress of an epidemic in a network where the connectivity of each individual changed over time, modelling the effects of political decisions made concerning various degrees of quarantine. It was published on December 23 in Europhysics Letters.
The authors stated: “Recently, several authors incorporated quarantine into COVID-19 modeling. However, these models were not network-based. In addition, they did not address the question of the optimal strategy for easing the quarantine in order to minimize the net number of infected individuals – one of the central questions in the present paper.” The benefits of a network-based model are that it more accurately accounts for a peaked distribution of individual disease durations, which is a problem for continuum models; also, it does not require the assumption of an equal number of contacts for each individual, so it more accurately models the underlying microscopic structure of the social network.
According to the authors, if a population has a homogeneous distribution of the number of contacts, “the total number of infected people at the end of the epidemic is the same as if no lockdown had been decreed (saturation of the health system aside),” whereas in the case of diverse frequency of contacts, the overall number of infected individuals can be significantly smaller. The reason for this effect is simple. After the individuals with a large number of contacts (high-degree nodes) have acquired immunity, they prevent the propagation of the epidemic through them, thus, slowing-down the spread of the epidemic through the network. Therefore, the optimal timing to allow the low-degree nodes to increase connections (by lifting the lockdown) would be after the high-degree nodes have become immune; this will minimize the net number of infected individuals over the course of the epidemic.
Marsh & McLennan CEO expects mandatory Covid vaccinations to be very rare – CNBC
The following are foreign headlines with hyperlinks to the posts
Singapore Airlines rolls out a new digital health passport for passengers.
Covid resurgence in parts of Asia could threaten the region’s economic recovery
The following additional national and state headlines with hyperlinks to the posts
Lions coach to miss game due to COVID-19 protocols
Bipartisan, bicameral group urges Trump to sign COVID-19 relief package
11-Year-Olds Could Get Vaccines Without Parental Consent in DC
80 Workers at Two In-N-Out Restaurants Test Positive for COVID in One Month
43% of Americans Say Stimulus Checks Should Be $2,000 or More: Poll
A few N.Y.C. hospitals fumble the vaccine rollout, with lower-risk workers cutting in line.
Air travel is down 60 percent from last Christmas, but many people are still flying.
Disposable surgical masks best for being heard clearly when speaking, study finds
Trump’s veto threat is holding up $9 billion in state vaccine funding
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
18 December 2020 ECRI’s WLI Growth Rate Continues To Improve
| Rail Week Ending 19 December 2020 – Strengthening Continues |
Warning to Readers
The amount of politically biased articles on the internet continues to increase. And studies and opinions of the experts continue to contradict other studies and expert opinions. Honestly, it is difficult to believe anything anymore. A study usually cannot establish cause and effect – but only correlation. Be very careful what you believe about this pandemic.

I assemble this coronavirus update daily – sifting through the posts on the internet. I try to avoid politically slanted posts (mostly from CNN, New York Times, and the Washington Post) and can usually find unslanted posts on that subject from other sources on the internet. I wait to publish posts on subjects that I cannot validate across several sources. But after all this extra work, I do not know if I have conveyed the REAL facts. It is my job to provide information so that you have the facts necessary – and then it is up to readers to draw conclusions.
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19 when recovering from COVID-19. Herd immunity does not look like an option without immunization although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a significantly higher death rate as there is relatively few hospitalizations and deaths in younger age groups..
- There are at least 8 strains of the coronavirus. New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
What we do or do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work.
- Do we develop lasting immunity to the coronavirus? Another coronavirus – the simple cold – does not develop long term immunity.
- To what degree do people who never develop symptoms contribute to transmission? Research early in the pandemic suggested that the rate of asymptomatic infections could be as high as 81%. But a meta-analysis, which included 13 studies involving 21,708 people, calculated the rate of asymptomatic presentation to be 17%.
- The accuracy of rapid testing is questioned – and the more accurate test results are not being given in a timely manner.
- Can children widely spread coronavirus? [current thinking is that they are a minor source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- Air conditioning contributes to the pandemic spread.
- It appears that there is increased risk of infection and mortality for those living in larger occupancy households.
- Male patients have almost three times the odds of requiring intensive treatment unit (ITU) admission compared to females.
- Outdoor activities seem to be a lower risk than indoor activities.
- Will other medical treatments for Covid-19 ease symptoms and reduce deaths? So far only remdesivir, Bamlanivimab,
and Regeneron) are approved for treatment. What drugs work?
- A current scientific understanding of the way the coronavirus works can be found [here].
There is now a vaccine available – the questions remain:
- how effective it will be in the general population,
- will there be any permanent side effects that will appear months from now,
- how long immunity will last [we can currently say we do not know if it will last more than 4 months],
- there is no evidence the vaccine will block transmission
Heavy breakouts of coronavirus have hit farmworkers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>




