
Written by Steven Hansen
The U.S. new cases 7-day rolling average is 19.3 % HIGHER than the 7-day rolling average one week ago. U.S. deaths due to coronavirus are now 11.0 % HIGHER than the rolling average one week ago. At the end of this post is a set of interactive graphs and tables for the world and individual States – as well as today’s headlines which include;
- The U.S. 7 day rolling average of new cases is at record levels – nearly 70,000
- COVID Can Age the Brain by a Decade
- Russia imposes a nationwide mask mandate
- Vaccine Hopes Rise as Oxford Jab Prompts Immune Response Among Old as Well as Young Adults
- Low risk or dicey? Two new reports paint different pictures of COVID-19 danger while flying
- Third wave of coronavirus infections in the U.S.? More like ‘wildfire’
- Nursing homes still don’t have enough PPE
- Two new reports paint different pictures of COVID-19 danger while flying
- What Are the Most Popular COVID-19 Tests?

The recent worsening of the trendlines for new cases should be attributed to going back to college/university, cooler weather causing more indoor activities, fatigue from wearing masks / social distancing, holiday activities, and continued loosening of regulations designed to slow the coronavirus spread.
My continuing advice is to continue to wash your hands, wear masks, avoid crowds, and maintain social distancing. No handwashing, mask, or social distancing will guarantee you do not get infected – but it sure as hell lowers the risk in all situations – as the evidence to-date shows a lower severity of COVID-19. In addition, certain activities are believed to carry higher risk – like being inside in air conditioning and removing your mask (such as restaurants, around your children/grandchildren, bars, and gyms). It is all about viral load – and outdoor activities are generally safe.
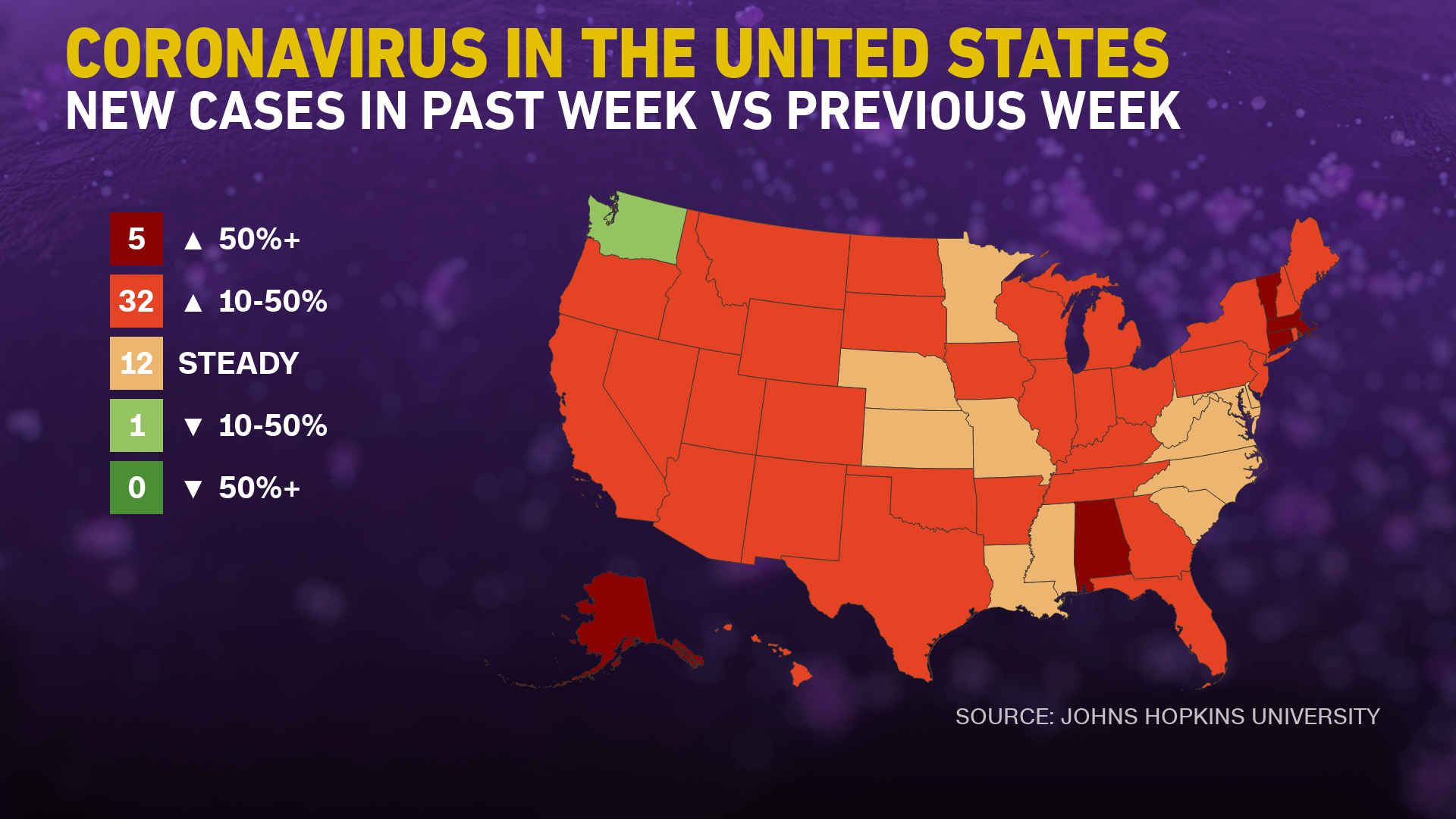
The daily number of new cases in the U.S. is remaining stubbornly and embarrassedly high.
include($_SERVER[‘DOCUMENT_ROOT’].’/pages/coronavirus1.htm’); ?>
Hospitalizations (grey line) and Mortality (green line) For Week ending 17OCT2020
source: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html
![]()
Coronavirus News You May Have Missed
COVID Can Age the Brain by a Decade, Study Suggests – Newsweek
COVID-19 may cause some people’s brains to age by around 10 years when compared with those who have not had the disease, according to a preliminary study.
Over 84,000 people in the U.K. who said they had recovered from a suspected or confirmed case of COVID-19 completed a questionnaire that measured their thinking skills. The paper was submitted to the preprint server medRxiv, meaning it has not been through the rigorous peer review process that is required for publication in a scientific journal, so the findings should be interpreted with caution.
The participants took tests to measure their ability to solve problems, spatial memory, attention, and how they processed emotions.
Immunity from the coronavirus may be steadily wearing off – Imperial College London
We observe a significant decline in the proportion of the population with detectable antibodies over three rounds of national surveillance, using a self-administered lateral flow test, 12, 18 and 24 weeks after the first peak of infections in England. This is consistent with evidence that immunity to seasonal coronaviruses declines over 6 to 12 months after infection and emerging data on SARS-CoV-2 that also detected a decrease over time in antibody levels in individuals followed in longitudinal studies. We observed clear differences in rates of decline between groups, for example those reporting SARS-CoV-2 infection based on PCR versus those without a history of COVID-19. In some groups with continued exposure risks no change in prevalence was seen (e.g. healthcare workers). The relevance of antibody waning for the potential for reinfection by SARS CoV-2 is currently not resolved. During any antibody response to an acute pathogen, some level of antibody waning in the months following infection is expected as short lived plasma cells die.
[editor’s note: this was a a study of more than 365,000 randomly selected people in England which found more than 26% saw a decline in COVID-19 antibodies over three months. “We know seasonal colds can reinfect people every six months,” Wendy Barclay, head of the infectious disease department at Imperial College London, told Politico, noting that the coronavirus appears to follow a similar trend. Another post on this subject A study finds declining antibodies in Britain, but experts say it’s not cause for concern.]
Nursing homes still don’t have enough PPE, study says – Philadelphia Inquirer
N95 and surgical masks, the backbone of protection against viruses in medical facilities, were still in short supply in many nursing homes at the end of the summer, according to a new analysis of federal data.
A report released Tuesday by the nonprofit U.S. PIRG Education Fund found that a fifth of nursing homes in late August had less than a week’s supply of some type of critical personal protective equipment (PPE). That is considered a dangerously low supply. The new report used data submitted by nursing homes to the U.S. Centers for Medicare & Medicaid Services.
Nursing home residents have been especially hard hit by the pandemic. They account for less than 1% of the population but more than a quarter of deaths, the report said. The virus has caused more severe disease and death in the elderly and people with multiple health problems.
The report found that shortages of N95 and surgical masks, gowns, eye protection, gloves and hand sanitizer worsened over the summer. N95 masks do the best job of filtering out viruses. They were the hardest protective gear to procure, with close to 8% of nursing homes unable to get any in August and 17% with less than a week’s supply. Hand sanitizer and gloves were the easiest.
Low risk or dicey? Two new reports paint different pictures of COVID-19 danger while flying – USA Today
The airline industry’s latest study says flying during the coronavirus pandemic is less risky than eating out or grocery shopping, but a COVID-19 outbreak linked to a seven-hour flight to Ireland is raising renewed concerns about in-flight transmission.
A 187-page study by Harvard scientists released Tuesday concluded that air travel “is as safe as or substantially safer than the routine activities people undertake during these times.” The study points to the ventilation systems on planes that refresh the air every two to three minutes, and new measures including heavy-duty disinfecting, strict face mask enforcement and social distancing during boarding and deplaning. The Harvard researchers said the ventilation system in the cabin “effectively counters the proximity travelers are subject to during flights.”
It says those factors combine to reduce the risk of COVID-19 transmission on a plane to below that at grocery stores or restaurants. But the authors said there is further room for improvement to minimize the risk, including even better social distancing when boarding and exiting, and keeping airplane ventilation systems on when the plane is parked at the gate, a practice not in place at all U.S. airlines.
The relatively rosy report from the Harvard T.H. Chan School of Public Health’s new Aviation Public Health Initiative, paid for by airlines, airplane manufacturers and airports, came to similar conclusions as recent studies promoted or sponsored by the industry.
… Despite the industry’s bullishness, a new report from Irish public health officials suggests coronavirus spread on planes remains a threat.
A report published late last week in the journal of the European Centre for Disease Prevention and Control, a European Union health agency, said 13 of 49 passengers on a 7½-hour flight to Dublin, including a child, tested positive for COVID-19, and another 46 in contact with them in Ireland became infected. Four were hospitalized, one in the ICU.
“This outbreak demonstrates the potential for spread of SARS-CoV-2 linked to air travel,” the report says, while noting that researchers don’t know whether the affected passengers were infected in-flight, during a connection, or before the flight. SARS-CoV-2 is severe acute respiratory syndrome coronavirus 2, the virus responsible for COVID-19.
Still, it says, this study is “one of few thus far demonstrating in-flight transmission of SARS-CoV-2 with extensive onwards transmission.”
Third wave of coronavirus infections in the U.S.? More like ‘wildfire,’ epidemiologist says – NBC News
During an outbreak, a “wave” comes from the curve used to visualize the number of people infected. If more people get sick every day, the curve goes up. If fewer people get sick every day, the curve goes down. Even during the summer, experts say cases in the U.S. never got to a low-enough level of new cases to make it out of the first wave from the spring when cases rose astronomically.
… “I look at it more as an elongated exacerbation of the original first wave,” Dr. Anthony Fauci, director of the National Institute for Allergy and Infectious Diseases, said Monday at an annual event for Yahoo Finance. “It’s kind of semantics. You want to call it the third wave or an extended first wave, no matter how you look at it, it’s not good news.”
Fauci and other experts are particularly concerned that the recent surge in cases is starting from a higher baseline of roughly 40,000 cases per day, compared with 20,000 cases per day during the summer surge.
“Each wave we start from a higher baseline and we start climbing,” Dr. Ashish Jha, dean of the Brown University School of Public Health said, noting that during the summer, infections were rising most in the South and Southwest. “This time, it’s all around the country and we’re heading into winter, where the virus becomes more efficient in spreading.”
Still, Jha said the terminology isn’t as important as Americans understanding that the growth of new cases can quickly become exponential.
“The metaphor of a wildfire is probably better,” said William Hanage, an associate professor of epidemiology at Harvard T.H. Chan School of Public Health. “It’s indisputable that the U.S. is now seeing a pretty widespread transmission across the board.”
Unlike a wave, which comes and passes through, wildfires can be patchy and more intense in areas, similar to the situation in the U.S., Hanage said. Community mitigation efforts such as masking and social distancing can stamp out the spread, but then infections tend to pop up in other areas with more relaxed measures.
What Are the Most Popular COVID-19 Tests? – MedPage
The FDA has authorized nearly 230 diagnostic tests for COVID-19, but which ones are most commonly used? Through interviews with companies, lab directors and pathologists, MedPage Today has compiled a list of key players.
We’ve grouped them by molecular versus antigen tests. Molecular tests identify viral RNA (frequently, but not always, through PCR testing), while antigen tests detect viral surface proteins. Either type can yield “rapid” tests, but antigen tests are inherently faster.
However, antigen tests are not as sensitive as molecular tests, carrying a greater chance of false negatives. Indeed, the emergency use authorization for each of the antigen tests indicates use in symptomatic patients only.
… A key to the information below: EUA = emergency use authorization; IFU = instructions for use. All sensitivity/specificity figures are manufacturer-reported and based on strict adherence to protocols for sample collection and handling. Note that result turnaround times specify only how long it takes to obtain results after a sample is placed in the analyzer; it does not account for sample transportation, in-lab backlogs in processing samples, or reporting of results, which often make for significant delay. Serology tests for anti-coronavirus antibodies are not covered here.
Molecular Tests
- Abbott IDNow: EUA; IFU; sensitivity/specificity: 100%/100%; results in 13 minutes
- Roche Cobas: EUA; IFU; sensitivity/specificity: 100%/100%; results in 3.5 hours
- Hologic Panther: EUA; IFU; sensitivity/specificity: 100%/100%; results in 3 hours
- Cepheid GeneXpert Xpress: EUA; IFU; sensitivity/specificity: 97.8%/95.6%; results in 45 minutes
- Thermo Fisher TaqPath: EUA; IFU; sensitivity/specificity: 100%/100%; results in 4 hours
- Labcorp: EUA; IFU; sensitivity/specificity: 100%/100%; results in 24 hours
- Quest Diagnostics: EUA; IFU; sensitivity/specificity: 100%/100%; results in 1 hour
Antigen Tests
- Abbott BinaxNOW: EUA; IFU; sensitivity/specificity: 97.1%/98.5%; results in 15 minutes
- Quidel Sofia: EUA; IFU; sensitivity/specificity: 96.7%/100%; results in 15 minutes
- BD Veritor: EUA; IFU; sensitivity/specificity: 84%/100%; results in 15 minutes
- Access Bio CareStart: EUA; IFU; sensitivity/specificity: 88.4%/100%; results in 10 minutes
- LumiraDx Ag: EUA; IFU; sensitivity/specificity: 97.6%/96.6%; results in 12 minutes
Vaccine Hopes Rise as Oxford Jab Prompts Immune Response Among Old as Well as Young Adults – Reuters
One of the world’s leading COVID-19 experimental vaccines produces a immune response in both old and young adults, raising hopes of a path out of the gloom and economic destruction wrought by the novel coronavirus.
The vaccine, developed by the University of Oxford, also triggers lower adverse responses among the elderly, British drug maker AstraZeneca Plc, which is helping manufacture the vaccine, said on Monday.
A vaccine that works is seen as a game-changer in the battle against the novel coronavirus, which has killed more than 1.15 million people, shuttered swathes of the global economy and turned normal life upside down for billions of people.
“It is encouraging to see immunogenicity responses were similar between older and younger adults and that reactogenicity was lower in older adults, where the COVID-19 disease severity is higher,” an AstraZeneca spokesman said.
Fact Check: Is a Mask Mandate Unconstitutional? – Newsweek
Mask mandates have riled some who consider the requirement to be an example of government overreach. They’ve held anti-mask rallies, spoken out on social media and filed lawsuits, arguing that the measure violates their constitutionally protected rights such as the First Amendment, the right to liberty and the right to privacy.
In accordance with the 10th Amendment, power that isn’t given to the federal government in the Constitution falls on the states, including responding to a public health crisis. So, as far as states having the power to implement a mask mandate, it likely would be upheld in court because the police power regulated to states have traditionally implied its ability to promote the public health and welfare of the general public.
As for a mask mandate violating someone’s personal liberty, there’s a 115-year-old precedent. In 1905, a citizen argued in the Jacobson v. Massachusetts case that a smallpox inoculation mandate infringed on his rights, but the Supreme Court upheld the Cambridge Board of Health’s authority to require the vaccine under the 10th Amendment.
In July, a Florida court pointed to the 1905 case in ruling that a mask ordinance did not violate any constitutional rights.
“In every well-ordered society charged with the duty of conserving the safety of its members the rights of the individual in respect of his liberty may at times, under the pressure of great dangers, be subjected to such restraint, to be enforced by reasonable regulations, as the safety of the general public may demand,” Circuit Court Judge John Kastrenakes wrote in his ruling, quoting the Jacobson opinion.
Russia imposes a nationwide mask mandate as its foreign minister, Sergey Lavrov, heads into quarantine. – New York Times
The Russian government on Tuesday made its most aggressive move yet to try to stem a second wave of the coronavirus, mandating masks in public places throughout the country.
The federal health watchdog agency, Rospotrebnadzor, also urged the governors of Russia’s 85 regions to order restaurants and entertainment venues to close by 11 p.m. Masks must be worn in taxis, public transportation, elevators and parking garages, and in any place where more than 50 people are able to gather, according to the order published on the watchdog’s website. Officials offered no immediate details on how the order would be enforced.
The directive was unusual because President Vladimir V. Putin has resisted taking any nationwide measures to stop the virus’s spread in recent months, delegating the battle to regional leaders. And after a nationwide lockdown in April and May caused widespread economic pain, officials have been loath to order any new business closures, even as the infection rate reached new heights in recent weeks.
In another measure of the virus’s spread, a number of top officials have been exposed or infected. Sergey V. Lavrov, the foreign minister, entered self-quarantine Tuesday after having had contact with someone who tested positive for the virus. The speaker of the lower house of parliament, Vyacheslav V. Volodin, told Mr. Putin on Monday that 91 of the assembly’s 450 representatives have or have had the coronavirus — and that 38 are currently hospitalized with the infection.
The following are foreign headlines with hyperlinks to the posts
Italians turned out in several cities and towns to vent anger, sometimes violently, over the latest pandemic restrictions that force restaurants and cafes to close at 6 p.m. and shutter cinemas, gyms and other leisure venues.
Protesters in Italy and Spain clash with police as they call for ‘freedom’ from virus restrictions.
Dubai International Airport is getting busier but it’s a long way from what it once was.
India’s Daily Infections at Lowest in 3 Months
Europe Needs ‘Serious Acceleration’ in Fight Against Coronavirus: WHO
Belgian Hospitals Could Run Out of Intensive Care Beds in 15 Days
Russia Confirms Production of Second COVID-19 Vaccine
Reality bites for Putin’s much-hyped Covid-19 vaccine, as concerns over efficacy and safety linger
Potential COVID Outbreak at U.N. HQ as In-Person Meetings Canceled
Wuhan Doctor Whose Skin Turned Dark from COVID Now Back to Normal
Mexico City’s mayor tests positive as the city grapples with a surge in cases.
The European Union doesn’t expect to have enough vaccines for everyone in the 27-country bloc until 2022
New York City residents should avoid traveling out of state this holiday season as the Big Apple responds to the “real threat” of a second wave of coronavirus infections
Belgium on the brink as virus surge fills ICU beds
The following are additional national and state headlines with hyperlinks to the posts
Confirmed infections per day are rising in 47 states, and deaths are up in 34 states,
Fox News anchors quarantine after COVID-19 exposure
Lakers title run may have fed COVID-19 surge in LA
Eli Lilly said its investigational monoclonal antibody bamlanivimab — one of the agents used in treating former New Jersey Gov. Chris Christie — failed to improve outcomes in hospitalized COVID-19 patients.
CMS will announce a plan this week to make coronavirus vaccines free for Medicare and Medicaid recipients once the products are authorized.
Vice President Pence tested negative again on Monday, his office said, even as multiple close aides have become infected with the coronavirus.
U.S. News & World Report‘s 2020-2021 rankings of best nursing homes are out, and this year incorporates facilities’ COVID-19 infection rates.
After Petroleum County, Montana, reported its first few cases this month, only two counties remain untouched by the pandemic.
Amid an alarming rise in cases, the Utah Hospital Association presented Gov. Gary Herbert (R) with criteria for physicians to ration care if facilities become overwhelmed.
Early pandemic data on hospitalized healthcare professionals found that nearly three-fourths were obese, about a third were nurses, 28% landed in the ICU, and 4% died.
El Paso, Texas, Judge Issues 2-Week Curfew To Stem Surge Of COVID-19 Cases
Trump says stimulus deal will happen after election
Texas neck-and-neck with California for most COVID-19 cases
35,000 Attend Anti-Lockdown Pastor’s Maskless Concert in National Mall
Pfizer will not deliver vaccine results by the end of this month, its chief executive says.
A virus cluster erupts in the Arkansas Legislature and the state surgeon general’s family.
The economic recovery in New York City could be slower than in the rest of the U.S.
Novavax delays U.S. trial of Covid-19 vaccine candidate to November
3M is making more N95 masks than ever as global Covid cases rise, CEO says
Coronavirus slows pace of college tuition increases
Today’s Posts On Econintersect Showing Impact Of The Pandemic With Hyperlinks
October 2020 Conference Board Consumer Confidence Decreased Slightly in October
October 2020 Richmond Fed Manufacturing Survey Improvement Continues
Headline Durable Goods New Orders Improved Again In September 2020
Headline Durable Goods New Orders Improved Again In September 2020

Coronavirus Cases Increase In 44 States As Some Hospitals Buckle L GMA
Four Ways To Rescue The Economy From The Pandemic
Warning to Readers
The amount of politically biased articles on the internet continues to increase. And studies and opinions of the experts continue to contradict other studies and expert opinions. Honestly, it is difficult to believe anything anymore. A study usually cannot establish cause and effect – but only correlation. Be very careful what you believe about this pandemic.

I assemble this coronavirus update daily – sifting through the posts on the internet. I try to avoid politically slanted posts (mostly from CNN, New York Times, and the Washington Post) and can usually find unslanted posts on that subject from other sources on the internet. I wait to publish posts on subjects that I cannot validate across several sources. But after all this extra work, I do not know if I have conveyed the REAL facts. It is my job to provide information so that you have the facts necessary – and then it is up to readers to draw conclusions.
Analyst Opinion of Coronavirus Data
There are several takeaways that need to be understood when viewing coronavirus statistical data:
- The global counts are suspect for a variety of reasons including political. Even the U.S. count has issues as it is possible that as much as half the population has had coronavirus and was asymptomatic. It would be a far better metric using a random sampling of the population weekly. In short, we do not understand the size of the error in the tracking numbers.
- Just because some of the methodology used in aggregating the data in the U.S. is flawed – as long as the flaw is uniformly applied – you establish a baseline. This is why it is dangerous to compare two countries as they likely use different methodologies to determine who has (and who died) from coronavirus.
- COVID-19 and the flu are different but can have similar symptoms. For sure, COVID-19 so far is much more deadly than the flu. [click here to compare symptoms]
- From an industrial engineering point of view, one can argue that it is best to flatten the curve only to the point that the health care system is barely able to cope. This solution only works if-and-only-if one can catch this coronavirus once and develops immunity. In the case of COVID-19, herd immunity may need to be in the 80% to 85% range. WHO warns that few have developed antibodies to COVID-19. At this point, herd immunity does not look like an option although there is now a discussion of whether T-Cells play a part in immunity [which means one might have immunity without antibodies]
- Older population countries will have a higher death rate.
- There are at least 8 strains of the coronavirus. New York may have a deadlier strain imported from Europe, compared to less deadly viruses elsewhere in the United States.
- Each publication uses different cutoff times for its coronavirus statistics. Our data uses 11:00 am London time. Also, there is an unexplained variation in the total numbers both globally and in the U.S.
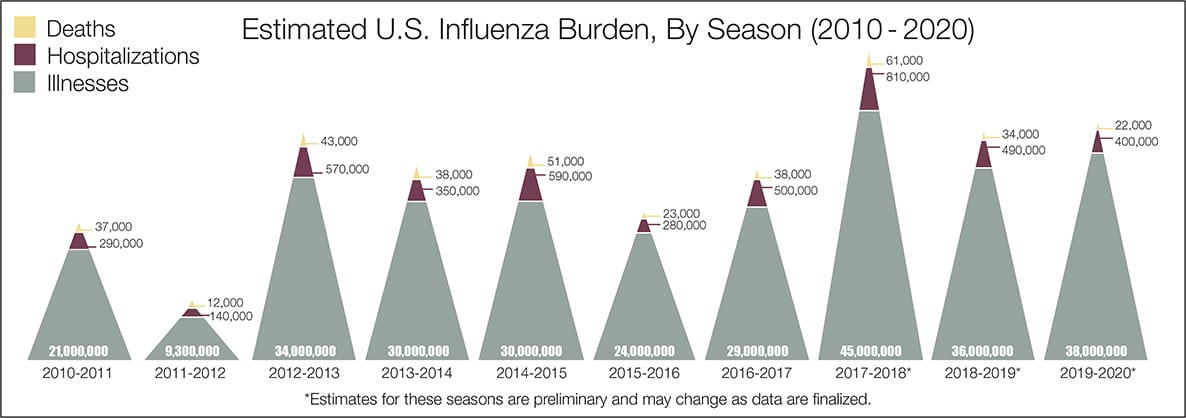
- The real question remains if the U.S. is over-reacting to this virus. The following graphic from the CDC puts the annual flu burden in perspective [click on image to enlarge]. Note that using this data is dangerous as the actual flu cases are estimated and not counted – nobody knows how accurate these guesses are.
What we do not know about the coronavirus [actually there is little scientifically proven information]. Most of our knowledge is anecdotal, from studies with limited subjects, or from studies without peer review.
- How many people have been infected as many do not show symptoms?
- Masks do work.
- Do we develop lasting immunity to the coronavirus? Another coronavirus – the simple cold – does not develop long term immunity.
- To what degree do people who never develop symptoms contribute to transmission?
- The US has scaled up coronavirus testing – and the accuracy of the tests has been improving. However, if one loses immunity – the coronavirus testing value is reduced.
- Can children widely spread coronavirus? [current thinking is that they are becoming a major source of the pandemic spread]
- Why have some places avoided big coronavirus outbreaks – and others hit hard?
- What effect will the weather have? At this point, it does not seem hot weather slows this coronavirus down – and it seems air conditioning contributes to its spread.
- Outdoor activities seem to be a lower risk than indoor activities.
- Can the world really push out an effective vaccine in 12 to 18 months?
- Will other medical treatments for Covid-19 ease symptoms and reduce deaths? So far only one drug (remdesivir) is approved for treatment.
- A current scientific understanding of the way the coronavirus works can be found [here].
Heavy breakouts of coronavirus have hit farm workers. Farmworkers are essential to the food supply. They cannot shelter at home. Consider:
- they have high rates of the respiratory disease [occupational hazard]
- they travel on crowded buses chartered by their employers
- few have health insurance
- they cannot social distance and live two to four to a room – and they eat together
- some reports say half are undocumented
- they are low paid and cannot afford not to work – so they will go to work sick
- they do not have access to sanitation when working
- a coronavirus outbreak among farmworkers can potentially shutter entire farm
The bottom line is that COVID-19 so far has been shown to be much more deadly than the data on the flu. Using CDC data, the flu has a mortality rate between 0.06 % and 0.11 % Vs. the coronavirus which to date has a mortality rate of 4 % [the 4% is the average of overall statistics – however in the last few months it has been hovering around 1.0%] – which makes it between 10 and 80 times more deadly. The reason for ranges:
Because influenza surveillance does not capture all cases of flu that occur in the U.S., CDC provides these estimated ranges to better reflect the larger burden of influenza.
There will be a commission set up after this pandemic ends to find fault [it is easy to find fault when a once-in-a-lifetime event occurs] and to produce recommendations for the next time a pandemic happens. Those that hate President Trump will conclude the virus is his fault.
Resources:
- Get the latest public health information from CDC: https://www.coronavirus.gov .
- Get the latest research from NIH: https://www.nih.gov/coronavirus.
- Find NCBI SARS-CoV-2 literature, sequence, and clinical content: https://www.ncbi.nlm.nih.gov/sars-cov-2/.
- List of studies: https://icite.od.nih.gov/covid19/search/#search:searchId=5ee124ed70bb967c49672dad
include(“/home/aleta/public_html/files/ad_openx.htm”); ?>




